



Correlation between function and imaging indexes after anatomic locking plate for proximal humeral fractures
-
摘要:
目的探索解剖锁定钢板(ALP)治疗肱骨近端骨折(PHF)术后功能与影像学指标之间的相关性。 方法回顾性分析2016年6月~2019年1月本院收治的120例PHF患者,根据患者的Neer分型将其分为二部分骨折组(n=28)、三部分骨折组(n=60)和四部分骨折组(n=32)。所有患者均采用ALP治疗,记录患者ALP的手术时间和术中出血量;术后1年,X线片检查患者颈干角丢失角度和肱骨头丢失高度,检查患肢肩关节的活动度,采用Constant-murley评分评估肩关节功能,视觉模拟评分评估术后疼痛程度,Pearson相关性分析PHF患者术后肩关节功能与颈干角丢失角度和肱骨头丢失高度之间的相关性。 结果随着Neer分型增加,PHF患者术中出血量明显增加(P < 0.05),术后颈干角丢失角度和肱骨头高度丢失明显增加(P < 0.05),肩关节前屈、外旋、内旋角度明显下降(P < 0.05),Constant评分明显降低(P < 0.05),视觉模拟评分明显增加(P < 0.05);Pearson相关性分析显示,PHF患者术后肩关节前屈、外旋、内旋、Constant评分与术后颈干角丢失角度和肱骨头高度呈显著的负相关关系(P < 0.05)。 结论PHF患者ALP术后肩关节活动度和功能与颈干角、肱骨头高度变化具有显著的相关性。 Abstract:ObjectiveTo explore the correlation between function and imaging indexes after anatomic locking plate (ALP) for proximal humeral fractures (PHF). MethodsA retrospective analysis was performed on the 120 PHF patients who were admitted to the hospital from June 2016 to January 2019. According to Neer classifications, they were divided into two-part fracture group (n=28), three-part fracture group (n=60) and four-part fracture group (n=32). All were treated with ALP. The operation time and intraoperative blood loss were recorded. At 1 year after surgery, loss angle of neck shaft angle, loss height of humeral head and range of motion (ROM) of effected shoulder joints were examined by X-ray films. The shoulder function was evaluated by Constant-murley scores. The postoperative pain was evaluated by scores of VAS. The correlation between postoperative function and imaging indexes in PHF patients was analyzed by Pearson correlation analysis. ResultsWith the increase of Neer classification, intraoperative blood loss was significantly increased in PHF patients (P < 0.05), postoperative loss angle of neck shaft angle and loss height of humeral head were significantly increased (P < 0.05), anteflexion, external and internal rotation angles of shoulder joints and Constant scorewere significantly decreased (P < 0.05), and VAS score was significantly increased (P < 0.05). Pearson correlation analysis showed that postoperative anteflexion, external rotation and internal rotation of shoulder joints, and Constant score were significantly negatively correlated with postoperative loss angle of neck shaft angle and loss height of humeral head (P < 0.05). ConclusionROM of shoulder joints is significantly correlated with changes in neck shaft angle and height of humeral head in PHF patients after ALP. -

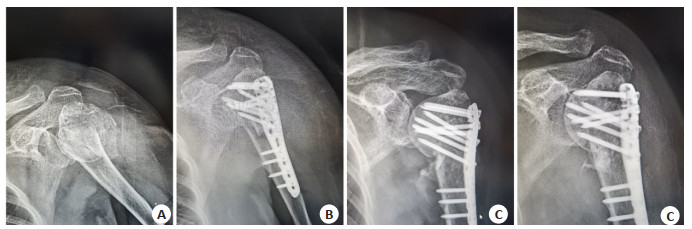
图 1 PHF患者术后的影像学参数
A~D来源于同一患者.A:术前; B:术后1周; C:术后3月; D:术后1年.
Figure 1. Postoperative imaging parameters in PHF patients.
表 1 PHF患者手术的一般情况
Table 1. General conditions of surgery in PHF patients (Mean±SD)
组别 手术时间(min) 术中出血量(mL) 二部分骨折组(n=28) 92.72±21.43 125.72±21.53 三部分骨折组(n=60) 96.85±22.81 176.64±30.87* 四部分骨折组(n=32) 105.26±26.54 238.47±57.22*# F 2.293 66.107 P 0.106 < 0.001 *P < 0.05 vs二部分骨折组; #P < 0.05 vs三部分骨折组. PHF: Proximal humeral fractures.  下载: 导出CSV
下载: 导出CSV
表 2 PHF患者术后的影像学参数
Table 2. Postoperative imaging parameters of PHF patients (Mean±SD)
组别 颈干角丢失角度(°) 肱骨头高度丢失(mm) 二部分骨折组(n=28) 2.63±0.71 1.67±0.42 三部分骨折组(n=60) 4.25±1.22* 2.52±0.68* 四部分骨折组(n=32) 6.37±1.54*# 3.74±0.91*# F 71.256 66.819 P < 0.001 < 0.001 *P < 0.05 vs二部分骨折组; #P < 0.05 vs三部分骨折组.
下载: 导出CSV
表 3 两组PHF患者术后肩关节的活动度
Table 3. ROM of shoulder joints in PHF patients(°, Mean±SD)
组别 前屈 外旋 内旋 二部分骨折组(n=28) 147.25±21.58 47.46±6.43 45.71±5.01 三部分骨折组(n=60) 134.76±15.64* 44.51±6.60* 42.80±4.93* 四部分骨折组(n=32) 127.22±13.50*# 40.29±5.52*# 40.03±4.86*# F 10.908 9.987 9.919 P < 0.001 < 0.001 < 0.001 *P < 0.05 vs二部分骨折组; #P < 0.05 vs三部分骨折组.
下载: 导出CSV
表 4 各组ONFH患者术后髋关节VAS和HSS评分
Table 4. Postoperative scores of VAS and HSS in ONFH patients of each group (score, Mean±SD)
组别 Constant评分 VAS 二部分骨折组(n=28) 88.44±7.63 1.24±0.31 三部分骨折组(n=60) 84.49±9.58 1.37±0.30 四部分骨折组(n=32) 80.42±10.21*# 1.45±0.32* F 5.517 3.529 P 0.005 0.033 *P < 0.05 vs二部分骨折组; #P < 0.05 vs三部分骨折组.
下载: 导出CSV
表 5 PHF患者术后功能与术后影像学之间的相关性分析
Table 5. Correlation between postoperative function and imaging in PHF patients
指标 颈干角丢失角度 肱骨头高度丢失 前屈 r=-0.421* r=-0.382* 外旋 r=-0.417* r=-0.364* 内旋 r=-0.406* r=-0.357* Constant评分 r=-0.434* r=-0.387* VAS r=0.121# r=0.165# *P < 0.001; #P>0.05
下载: 导出CSV
-
[1] Pogorelić Z, Kadić S, Milunović KP, et al. Flexible intramedullary nailing for treatment of proximal humeral and humeral shaft fractures in children: a retrospective series of 118 cases[J]. Orthop Traumatol Surg Res, 2017, 103(5): 765-70. doi: 10.1016/j.otsr.2017.02.007 [2] Beks RB, Ochen Y, Frima H, et al. Operative versus nonoperative treatment of proximal humeral fractures: a systematic review, metaanalysis, and comparison of observational studies and randomized controlled trials[J]. J Shoulder Elbow Surg, 2018, 27(8):1526-34. doi: 10.1016/j.jse.2018.03.009 [3] 谢继勇, 谭响, 皮昌军, 等.锁定钢板治疗老年肱骨近端骨折的疗效[J].中华创伤杂志, 2017(5):414-8. doi: 10.3760/cma.j.issn.1001-8050.2017.05.006 [4] Lopiz Y, Alcobía-Díaz B, Galán-Olleros M, et al. Reverse shoulder arthroplasty versus nonoperative treatment for 3-or 4-part proximal humeral fractures in elderly patients: a prospective randomized controlled trial[J]. J Shoulder Elbow Surg, 2019, 28(12): 2259-71. doi: 10.1016/j.jse.2019.06.024 [5] Cha H, Park KB, Oh S, et al. Treatment of comminuted proximal humeral fractures using locking plate with strut allograft[J]. J Shoulder Elbow Surg, 2017, 26(5): 781-5. doi: 10.1016/j.jse.2016.09.055 [6] 李旭, 李奉龙, 鲁谊, 等.锁定钢板治疗非骨质疏松性复杂肱骨近端骨折的中期临床及影像学随访研究[J].北京大学学报(医学版), 2017, 49(5): 855-60. doi: 10.3969/j.issn.1671-167X.2017.05.020 [7] Mahadeva D, MacKay DC, Turner SM, et al. Reliability of the neer classification system in proximal humeral fractures: a systematic review of the literature[J]. Eur J Orthop Surg Traumatol, 2008, 18(6): 415-24. doi: 10.1007/s00590-008-0325-6 [8] Çelik D. Turkish version of the modified Constant-Murley score and standardized test protocol: reliability and validity[J]. Acta Orthop Traumatol Turc, 2016, 50(1): 69-75. https://pubmed.ncbi.nlm.nih.gov/26854052/ [9] Reich A, Heisig M, Phan NQ, et al. Visual analogue scale: evaluation of the instrument for the assessment of pruritus[J]. Acta Derm Venereol, 2012, 92(5): 497-501. doi: 10.2340/00015555-1265 [10] Beeres FJP, Quaile OM, Link BC, et al. Reduction techniques for minimally invasive stabilization of proximal humeral fractures[J]. Oper Orthop Traumatol, 2019, 31(1): 63-80. doi: 10.1007/s00064-018-0586-0 [11] Thienthong K, Boonard M, Boonrod A, et al. Cadaveric study of the anatomical reference points for proximal humeral plate positioning [J]. Eur J Orthop Surg Traumatol, 2018, 28(7): 1269-72. doi: 10.1007/s00590-018-2208-9 [12] 王海燕, 许贵存, 蔡永强, 等.胫骨远端骨折解剖锁定钢板固定的有限元分析[J].中国组织工程研究, 2017, 820(35): 121-6. http://www.cnki.com.cn/Article/CJFDTOTAL-XDKF201735021.htm [13] 岳宪虎, 孙付杰, 张振华, 等.锁骨解剖锁定钢板对不稳定锁骨骨折患者肩关节功能的影响[J].中华保健医学杂志, 2015, 17(6): 454-5. [14] 曾周景, 叶建华, 谭通, 等.肱骨近端骨折锁定钢板内固定术后影响肩关节功能的相关因素分析[J].中国矫形外科杂志, 2016, 24(16): 1462-5. http://www.cnki.com.cn/Article/CJFDTotal-ZJXS201616008.htm [15] Huang SG, Chen B, Lv D, et al. Evaluation of shoulder function in clavicular fracture patients after six surgical procedures based on a network meta-analysis[J]. Disabil Rehabil, 2017, 39(2): 105-12. doi: 10.3109/09638288.2016.1140827 [16] 杨立文, 鞠文, 翁峰标, 等.锁定钢板治疗老年性肱骨近端骨折52例疗效分析[J].中国矫形外科杂志, 2017, 25(14): 1328-31. http://www.cnki.com.cn/Article/CJFDTOTAL-ZJXS201714018.htm [17] Zhao L, Qi YM, Yang L, et al. Comparison of the effects of proximal humeral internal locking system (PHILOS) alone and PHILOS combined with fibular allograft in the treatment of neer three-or fourpart proximal humerus fractures in the elderly[J]. Orthop Surg, 2019, 11(6): 1003-12. doi: 10.1111/os.12564 [18] 赵洪斌, 宋洋, 黄明光, 等.锁定钢板治疗不同Neer分型肱骨近端骨折的疗效及生物力学恢复情况的评价[J].中国全科医学, 2019, 22 (32):3985-9. doi: 10.12114/j.issn.1007-9572.2019.00.433 [19] Malavolta EA, Assunção JH, Gracitelli MEC, et al. Correlation between the UCLA and Constant-Murley scores in rotator cuff repairs and proximal humeral fractures osteosynthesis[J]. Rev Bras Ortop, 2018, 53(4): 441-7. doi: 10.1016/j.rbo.2017.10.003 [20] 唐芳根, 金丹, 黎健伟.数字化重建技术在肱骨近端骨折临床分型中的应用[J].南方医科大学学报, 2012, 32(11): 1671-4. doi: 10.3969/j.issn.1673-4254.2012.11.034 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 492
- HTML全文浏览量: 313
- PDF下载量: 8
- 被引次数: 0