



Etiology and clinical analysis of hemoptysis in patients with previous pulmonary tuberculosis history
-
摘要:
目的分析既往有肺结核病史患者咯血的病因及临床特点,为该类患者的诊治提供参考。 方法回顾性分析广州市胸科医院2018年1~12月既往有肺结核病史、以咯血为主诉的182例住院患者的相关临床资料,其中男性145例,女性37例,年龄55.13±13.73岁。分析其影像学改变、支气管镜检查、病原学等结果,总结病因及临床特点。 结果既往患肺结核治愈后至本次咯血发生的时间为10.13±8.29年。咯血的主要病因是肺结核后空洞继发曲菌球(23.63%),其次是支气管扩张和肺结核复发(23.08%)、肺炎(19.23%)及NTM肺病(8.79%),少数是肺部肿瘤(1.65%)、支气管异物(0.55%)。 结论既往有肺结核病史的患者咯血绝大部分与肺的结构破坏有关,肺结核复发只是其中的病因之一,不能单凭既往有过肺结核病史和影像学改变,就诊断为肺结核复发,容易造成误诊、漏诊及误治。建议综合临床资料全面进行分析,从常见病因入手,尽量利用现有的医疗技术寻找确诊证据,同时应警惕一些少见或罕见病因。 Abstract:ObjectiveSummarize and analyze the etiology and clinical characteristics of hemoptysis of patients with previous history of pulmonary tuberculosis to provide reference for the diagnosis and treatment of them. MethodsThe clinical data of 182 inpatients with a history of pulmonary tuberculosis and hemoptysis were retrospectively analyzed in Guangzhou Chest Hospital from January to December 2018, including imaging changes, bronchoscopy, etiology and other results. And the etiology and clinical characteristics were summarized. A total of 182 patients were included, 145 males and 37 females, with an average age at 55.13±13.73 years old. ResultsThe average time from cure of tuberculosis to hemoptysis was 10.13±8.29 years. The main causes of hemoptysis were pulmonary tuberculosis posterior cavity secondary aspergilloma (23.63%), followed by bronchiectasis and pulmonary tuberculosis recurrence (23.08%), pneumonia (19.23%) and NTM lung disease (8.79%). A few of them were lung tumor (1.65%) and bronchial foreign body (0.55%). ConclusionMost of hemoptysis in patients with a history of pulmonary tuberculosis is related to the structural damage of the lung. The recurrence of pulmonary tuberculosis is only one of the causes. The diagnosis of pulmonary tuberculosis recurrence can not just base on the past history of pulmonary tuberculosis and imaging changes. It is easy to cause misdiagnosis, missed diagnosis and mistreatment. It is suggested that comprehensive analysis of clinical data should be applied, starting from common causes, the existing medical technology should be used to find the evidence of diagnosis, and at the same time, some rare causes should be watched out for. -
Key words:
- pulmonary tuberculosis /
- hemoptysis /
- etiology /
- aspergilloma /
- bronchiectasis
-
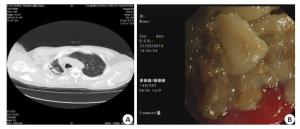
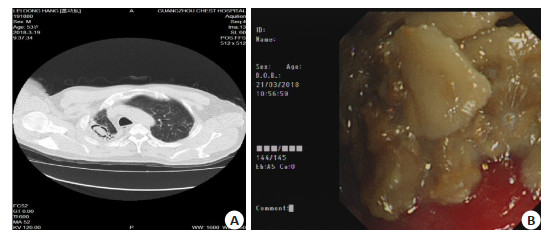
图 1 肺结核后空洞内继发曲菌球的CT及支气管镜表现
A:胸部CT显示典型的空气新月征; B:支气管镜下见空洞内大量土黄色块状坏死物堆积.
Figure 1. CT and bronchoscopy of secondary aspergilloma in pulmonary tuberculosis.
表 1 肺结核治愈后出现咯血的时间(n)
Table 1. The time of hemoptysis after cure of pulmonary tuberculosis
患者分类* 咯血时间(年) 5 10 15 20 25 30 35 40 青年 19 8 3 6 - - - - 中年 21 22 8 12 3 2 1 1 老年 30 22 7 8 3 4 0 2 总体 70 52 18 26 6 6 1 3 *按世界卫生组织标准, ≤44岁为青年, 45~59岁为中年, ≥60岁为老年.  下载: 导出CSV
下载: 导出CSV
表 2 不同病因咯血量情况及构成比[n(%)]
Table 2. Hemoptysis volume and constituent ratio of different causes
病因 少量咯血 中量咯血 大量咯血 合计 肺曲菌球 26(60.47) 15(34.88) 2(4.65) 43(23.63) 支扩并感染 29(69.05) 12(28.57) 1(2.38) 42(23.08) 肺结核复治 28(66.67) 10(23.81) 4(9.52) 42(23.08) 肺炎 25(71.43) 8(22.86) 2(5.71) 35(19.23) NTM肺病 10(62.50) 3(18.75) 3(18.75) 16(8.79) 肺癌 2(66.67) 1(33.33) 0(0) 3(1.65) 支气管异物 1(100.00) 0(0) 0(0) 1(0.55) 合计 121(66.48) 49(26.92) 12(6.59) 182(100.00) NTM: Nontuberculous mycobacteria.
下载: 导出CSV
表 3 不同年龄段各类咯血病因的分布[n(%)]
Table 3. Distribution of causes of hemoptysis in different age groups
患者分类 肺曲菌球 支扩并感染 肺结核复治 肺炎 NTM肺病 肺癌 支气管异物 合计 青年 8(22.22) 8(22.22) 15(41.67) 4(11.11) 1(2.78) 0(0) 0(0) 36(19.78) 中年 21(30.00) 10(14.29) 16(22.86) 17(24.29) 6(8.57) 0(0) 0(0) 70(38.46) 老年 14(18.42) 24(31.58) 11(14.47) 14(18.42) 9(11.84) 3(3.95) 1(1.32) 76(41.76) 合计 43(23.63) 42(23.08) 42(23.08) 35(19.23) 16(8.79) 3(1.65) 1(0.55) 182(100.00)
下载: 导出CSV
表 4 不同病因血液检查结果[n(%)]
Table 4. Blood examination results of different causes
病因 血像升高 C反应蛋白升高 降钙素原升高 纤维蛋白原减少 IGRAs阳性 肺曲菌球(n=43) 18(41.86) 23(53.49) 8(18.60) 3(6.98) 17(39.53) 支扩并感染(n=42) 20(47.62) 31(73.81) 11(26.19) 8(19.05) 10(23.81) 肺结核复治(n=42) 14(33.33) 16(38.10) 7(16.67) 4(9.52) 32(76.19) 肺炎(n=35) 11(31.43) 11(31.43) 2(5.71) 5(14.29) 22(62.86) NTM肺病(n=16) 4(25.00) 6(37.50) 3(18.75) 0(0) 2(12.50) 肺癌(n=3) 1(33.33) 3(100.00) 0(0) 0(0) 1(33.33) 支气管异物(n=1) 0(0) 0(0) 0(0) 0(0) 0(0) 合计 68(37.36) 90(49.45) 31(17.03) 20(10.99) 84(46.15) IGRA: Interferon gamma release assay.
下载: 导出CSV
表 5 不同病因病原菌检测阳性的结果[n(%)]
Table 5. Positive results of pathogenic bacteria in different causes
病因 抗酸染色涂片 Gene Xpert MTB/RIF* MTB NTM 细菌培养 真菌培养 肺曲菌球(n=43) 0(0) 2(4.76) 0(0) 0(0) 7(16.28) 10(23.26) 支扩并感染(n=42) 0(0) 0(0) 0(0) 0(0) 11(26.19) 1(2.38) 肺结核复治(n=42) 30(71.43) 40(95.24) 37(88.10) 0(0) 0(0) 1(2.38) 肺炎(n=35) 0(0) 0(0) 0(0) 0(0) 5(14.29) 1(2.86) NTM肺病(n=16) 7(43.75) 0(0) 0(0) 16(100.00) 0(0) 0(0) 肺癌(n=3) 0(0) 1(33.33) 0(0) 0(0) 0(0) 0(0) 支气管异物(n=1) 0(0) 1(100.00) 0(0) 0(0) 1(100.00) 0(0) 合计 37(20.33) 44(24.18) 37(20.33) 16(8.79) 24(13.19) 13(7.14) *检测结核分枝杆菌rpoB基因及其突变的快速分子诊断技术;MTB: mycobacterium tuberculosis.
下载: 导出CSV
-
[1] 张聪, 杨雅吉, 邢西迁. 238例咯血患者支气管镜下特点与病因分析[J].国际呼吸杂志, 2019, 39(13): 990-4. http://d.wanfangdata.com.cn/periodical/gwyx-hxxt201913007 [2] Cordovilla R, Bollo E, Nuñez AA, et al. Diagnosis and Treatment of Hemoptysis[J].Arch Bronconeumol, 2016, 52(7): 368-77. https://www.sciencedirect.com/science/article/abs/pii/S1579212916300568 [3] 钟南山, 刘又宁.呼吸病学[M]. 2版.北京:人民卫生出版社, 2012. [4] Soares Pires F, Teixeira N, Coelho F, et al. Hemoptysis: etiology, evaluation and treatment in a university hospital[J]. Rev Port Pneumol, 2011, 17(1): 7-14. http://www.ncbi.nlm.nih.gov/pubmed/21251478 [5] Rali P, Gandhi V, Tariq C. Massive Hemoptysis[J]. Crit Care Nurs Q, 2016, 39(2): 139-47. [6] 中华人民共和国国家卫生和计划生育委员会.肺结核诊断WS 288— 2017[J].中国感染控制杂志, 2018, 17(7): 642-52. http://www.cnki.com.cn/Article/CJFDTotal-XFCR201801019.htm [7] Denning DW, Cadranel J, Beigelman-Aubry C, et al. Chronic pulmonary aspergillosis: rationale and clinical guidelines for diagnosis and management[J]. Eur Respir J, 2016, 47(1): 45-68. [8] 成人支气管扩张症诊治专家共识编写组.成人支气管扩张症诊治专家共识[J].中华结核和呼吸杂志, 2012, 35(7): 485-92. http://www.cqvip.com/QK/89531X/201205/44229745.html [9] 中华医学会呼吸病学分会.中国成人社区获得性肺炎诊断和治疗指南(2016年版)[ J].中华结核和呼吸杂志, 2016, 39(4):253-79. [10] 北京医师协会呼吸内科专科医师分会咯血诊治专家共识编写组.咯血诊治专家共识[J].中国呼吸与危重监护杂志, 2020, 19(1): 1-11. http://www.cqvip.com/QK/85488X/202001/7100907435.html [11] 万春, 王锟琨, 文富强, 等.单中心418例成人咯血患者临床特点分析[J].西部医学, 2018, 30(7): 971-8. http://www.cqvip.com/QK/87101X/20187/675564845.html [12] Earwood JS, Thompson TD. Hemoptysis: evaluation and management[J].Am Fam Physician, 2015, 91(4): 243-9. http://smartsearch.nstl.gov.cn/paper_detail.html?id=52fe237193264b1d0a970b17f06a3e16 [13] Abdulmalak C, Cottenet J, Beltramo G, et al. Haemoptysis in adults: a 5-year study using the French nationwide hospital administrative database[J]. Eur Respir J, 2015, 46(2): 503-11. http://www.ncbi.nlm.nih.gov/pubmed/26022949 [14] Bhalla A, Pannu AK, Suri V. Etiology and outcome of moderate-tomassive hemoptysis: Experience from a tertiary care center of North India[J]. Int J Mycobacteriol, 2017, 6(3): 307-10. http://europepmc.org/abstract/MED/28776532 [15] 汤春梅, 张言斌.正规抗结核治疗后肺结核患者再咯血原因分析[J].临床肺科杂志, 2005, 10(4): 441-2. http://www.cnki.com.cn/Article/CJFDTotal-LCFK200504028.htm [16] Achkar JM, Joseph G. Independent association of younger age with hemoptysis in adults with pulmonary tuberculosis[J]. Int J Tuberc Lung Dis, 2012, 16(7): 897-902. [17] Kang MJ, Kim JH, Kim YK, et al. 2018 Korean clinical imaging guideline for hemoptysis[J]. Korean J Radiol, 2018, 19(5): 866-71. http://www.ncbi.nlm.nih.gov/pubmed/30174475 [18] 李瀛.肺结核合并曲霉菌感染的CT表现及分析[J].现代诊断与治疗, 2015, 26(1): 157-8. http://www.cnki.com.cn/Article/CJFDTotal-XDZD201501103.htm [19] 肖海浩, 汤春梅, 苏铎华, 等.支气管镜在肺结核空洞继发曲菌球的诊断价值[J].岭南急诊医学杂志, 2020, 25(3): 255-7. http://d.wanfangdata.com.cn/periodical/lnjzyxzz202003016 [20] Singh SK, Tiwari KK. Etiology of hemoptysis: a retrospective study from a tertiary care hospital from northern Madhya Pradesh, India [J]. Indian J Tuberc, 2016, 63(1): 44-7. http://www.ncbi.nlm.nih.gov/pubmed/27235944 [21] Lee BR, Yu JY, Ban HJ, et al. Analysis of patients with hemoptysis in a tertiary referral hospital[J]. Tuberc Respir Dis, 2012, 73(2): 107- 14. https://pubmed.ncbi.nlm.nih.gov/23166543/ [22] Horne DJ, Kohli M, Zifodya JS, et al. Xpert MTB/RIF and Xpert MTB/RIF Ultra for pulmonary tuberculosis and rifampicin resistance in adults[J]. Cochrane Database Syst Rev, 2019, 6: CD009593. https://www.researchgate.net/publication/333663502_Xpert_MTBRIF_and_Xpert_MTBRIF_Ultra_for_pulmonary_tuberculosis_and_rifampicin_resistance_in_adults [23] 李多, 房坤, 王珏, 等.非结核分枝杆菌肺病的CT分型及其临床特征分析(附132例报告)[ J].中国防痨杂志, 2019, 41(2): 202-9. http://www.cnki.com.cn/Article/CJFDTotal-ZFLZ201902016.htm [24] Rasool G, Khan AM, Mohy-Ud-Din R, et al. Detection of Mycobacterium tuberculosis in AFB smear-negative sputum specimens through MTB culture and GeneXpert® MTB/RIF assay [J]. Int J Immunopathol Pharmacol, 2019, 33: 2058738419827174. [25] 黄艳君, 谭耀驹, 蔡杏珊, 等. γ-干扰素释放试验在肺结核与非结核分枝杆菌肺病诊断的价值[J].中国防痨杂志, 2015, 37(6): 607-10. http://d.wanfangdata.com.cn/periodical/zgflzz201506007 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 615
- HTML全文浏览量: 287
- PDF下载量: 4
- 被引次数: 0