



Radiation dose in patients with acute ischemic stroke
-
摘要:
目的分析急性缺血性脑卒中患者在介入诊疗中的受照剂量,探讨性别、年龄、病变部位以及诊疗方式等因素对辐射剂量的影响。 方法回顾性分析我院行介入治疗的急性缺血性脑卒中患者156例,最终纳入113例,随机配置的辐射监测系统记录透视时间(FT)、剂量面积乘积(DAP)、空气比释动能(AK)。分析性别、患者年龄(30~60岁组、60~80岁组、≥80岁组)、闭塞位置(前、后循环)以及血管开通技术对患者受照剂量的影响。 结果患者FT值7.94~97.41 min(24.0±14.4 min);DAP值1638~551959 mGy·cm2(137 422.8±107 778.1 mGy·cm2);AK值11~5726 mGy(1210.9±1070.8 mGy)。男性患者辐射剂量高于女性患者,DAP值、AK值差异有统计学意义(P<0.05);3个年龄组间各剂量值差异均无统计学意义(P>0.05);前、后循环闭塞患者所受剂量差异无统计学意义(P>0.05);单纯导管抽吸(ASPI)患者辐射剂量最低,导管抽吸结合支架取栓(ASPI+SR)以及支架植入术组的辐射剂量大于ASPI组,3个剂量值差异均有统计学意义(P<0.05)。 结论急性缺血性脑卒中患者所受辐射剂量差异较大,性别、血管开通方式均是影响辐射剂量的重要因素。因此,可能需要针对不同特征的患者采取更积极的防护措施。 Abstract:ObjectiveTo analyze the dose of radiation in patients with acute ischemic stroke and to explore the influence of gender, age, lesion location and diagnosis and treatment methods on radiation dose. MethodsA total of 156 patients with acute ischemic stroke who underwent interventional therapy in our hospital were retrospectively analyzed, and 113 cases were finally included. Fluoroscopy time (FT), dose area product (DAP) and air specific kinetic energy (AK) were recorded by a random radiation monitoring system. The effects of gender, age (30-60 years old group, 60-80 years old group and ≥80 years old group), occlusion position (anterior and posterior circulation) and vascular opening technology on radiation dose were analyzed. ResultsThe FT value of the patients ranged from 7.94 to 97.41 min, with an average value of 24.0±14.4 min. The DAP value of the dose area ranged from 1638 to 551 959 mGy · cm2, the average was 137 422.8±107 778.1 mGy · cm2. The AK value of the dose area ranged from 11 to 5726 mGy, the average was 1210.9 ± 1070.8 mGy. Compared with males, females had less radiation dose. The values of DAP and AK had significant difference (P < 0.05). There was no significant difference between the three age groups in the analysis of the variance of each dose (P>0.05). There was no significant difference in the dose received by patients with anterior and posterior circulation occlusion (P>0.05). Patients with single catheter aspiration (ASPI) had the lowest radiation dose. The radiation dose of the catheter aspiration combined with stent retriever (ASPI + SR) and the stent implantation group was larger than that of the catheter aspiration only, and the difference of the three dose values was statistically significant (P < 0.05). ConclusionThe radiation dose of patients with acute ischemic stroke varies greatly, and gender, the way of vascular opening are all important factors affecting the radiation dose. Therefore, more aggressive protective measures may be needed for patients with different characteristics. -
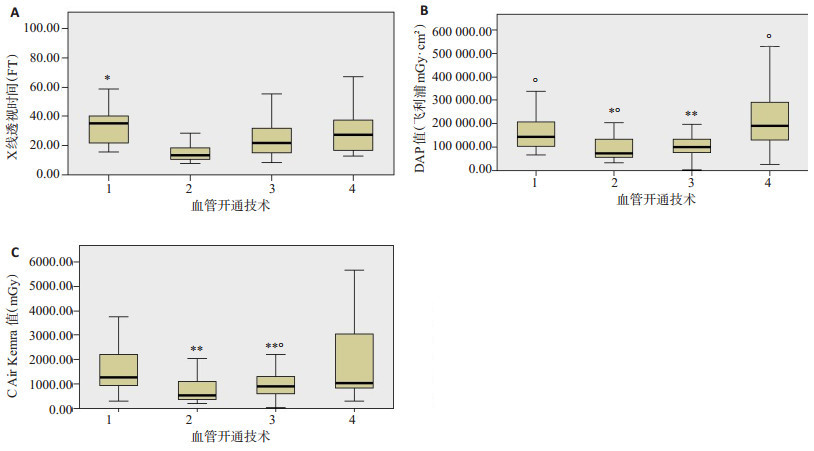
图 1 不同血管开通技术辐射剂量对比
4种血管开通技术的FT、DAP、AK值均值箱式图, 横坐标数字代表含义同表 5.A: 4种血管开通技术的FT值箱式图; B: 4种血管开通技术的DAP值箱式图; C: 4种血管开通技术的AK值箱式图.图示单纯ASPI组的辐射剂量最低
Figure 1. Comparison of radiation dose between different vascular opening techniques
表 1 患者的人口学/临床数据[n(%)]
Table 1. Information on demographic/clinical data among the patients
指标 数值 性别(男) 58 (51.33) 年龄(岁,Mean±SD) 68.0±12.70 责任血管 大脑中动脉M1~M2 59 (52.21) 大脑前动脉 7 (6.19) 颈内动脉 31 (27.43) 后循环 16 (14.16) 入院NIHSS评分(分,Mean±SD) 16.87±6.31 治疗相关 导管抽吸结合支架取栓(ASPI+SR) 18 (15.93) 导管抽吸(ASPI) 33 (29.20) 支架取栓(SR) 47 (41.59) 支架植入 15 (13.27) ASPI:Aspiration; SR: Stent retriever.  下载: 导出CSV
下载: 导出CSV
表 2 不同性别辐射剂量对比(Mean±SD)
Table 2. Comparison of radiation dose between different genders
性别 FT (min) DAP (mGy·cm2) AK (mGy) 男(n=58) 22.9±11.6 115114.1±118178.3 1420.8±1270.1 女(n=55) 25.2±15.8 118766.3±93059.3 989.5±760.3 t 0.967 1.995 2.220 P 0.336 0.049 0.028 FT: Fluoroscopy time; DAP: Dose area product; AK:Air kerma.
下载: 导出CSV
表 3 不同年龄段辐射剂量对比(Mean±SD)
Table 3. Comparison of radiation dose between different age groups
年龄组 FT (min) DAP (mGy·cm2) AK (mGy) 30~60岁(n=30) 25.0±13.0 153 908.4±116 503.7 1327.1±965.2 60~80岁(n=63) 23.0±15.9 140 429.8±116 042.1 1273.1±1230.3 ≥80岁(n=20) 25.4±11.2 103 222.2±46 106.8 840.4±1230.3 F 0.297 1.392 1.494 P 0.744 0.253 0.229
下载: 导出CSV
表 4 前循环和后循环辐射剂量对比(Mean±SD)
Table 4. Comparison of radiation dose between different occlusion locations
闭塞位置 FT (min) DAP (mGy·cm2) AK (mGy) 前循环(n=97) 24.0±14.1 131 701.4±98 388.2 1150.6±1006.2 后循环(n=16) 22.9±15.9 172 108.4±152 595.1 1576.2±1383.9 t 0.294 1.395 1.481 P 0.772 0.166 0.142
下载: 导出CSV
表 5 Kruskal-Wallis单因素ANOVA检验
Table 5. Kruskal-Wallis one-wayANOVAtest
变量 检验统计 标准误差 标准检验统计 显著性 调整后显著性 FT 2-3 -29.265 7.441 -3.933 0.000 0.001 2-4 -38, 058 10.203 -3.730 0.000 0.001 2-1 51.480 9.600 5.362 0.000 0.000 DAP 2-1 30.121 9.600 3.137 0.002 0.010 2-4 -37.521 10.203 -3.678 0.000 0.001 3-4 -27.081 9.716 -2.787 0.005 0.032 AK 2-1 31.902 9.600 3.323 0.001 0.005 2-4 -32.685 10.203 -3.204 0.001 0.008 注: 4种闭塞血管开通技术的FT、DAP、AK值组间两两对比结果, 图中数字代表各血管开通技术, 1: ASPI+SR; 2: ASPI; 3: SR; 4:支架植入.
下载: 导出CSV
-
[1] Wang WZ, Jiang B, Sun HX, et al. Prevalence, incidence, and mortality of stroke in China: results from a nationwide populationbased survey of 480 687 adults[J]. Circulation, 2017, 135(8): 759-71. doi: 10.1161/CIRCULATIONAHA.116.025250 [2] 中华医学会神经病学分会, 中华医学会神经病学分会脑血管病学组.中国急性缺血性脑卒中诊治指南2018[J].中华神经科杂志, 2018, 51 (9): 666-82. doi: 10.3760/cma.j.issn.1006-7876.2018.09.004 [3] Vergouwen MD, Algra A, Pfefferkorn T, et al. Time is brain(stem) in basilar artery occlusion[J]. Stroke, 2012, 43(11): 3003-6. doi: 10.1161/STROKEAHA.112.666867 [4] Khatri R, Vellipuram AR, Maud A, et al. Current endovascular approach to the management of acute ischemic stroke[J]. Curr Cardiol Rep, 2018, 20(6): 46. doi: 10.1007/s11886-018-0989-4 [5] 卢贤贵.全脑血管造影检查中患者X射线辐射评价与剂量控制方法[J].系统医学, 2016, 1(9): 68-70. [6] 张紫寅, 王德全, 段彬, 等.经桡动脉和股动脉路径行全脑血管造影和颈动脉支架置入术患者辐射剂量及照射时间研究[J].脑与神经疾病杂志, 2020, 28(4): 203-7. [7] 朱栋梁, 卢建华, 陈胜利, 等.脑血管介入造影检查中患者X射线辐射评价与剂量控制方法[J].生物医学工程与临床, 2012, 16(3): 246-9. doi: 10.3969/j.issn.1009-7090.2012.03.010 [8] Campbell BCV, Donnan GA, Lees KR, et al. Endovascular stent thrombectomy: the new standard of care for large vessel ischaemic stroke[J]. Lancet Neurol, 2015, 14(8): 846-54. doi: 10.1016/S1474-4422(15)00140-4 [9] Dávalos A, Cobo E, Molina CA, et al. Safety and efficacy of thrombectomy in acute ischaemic stroke (REVASCAT): 1-year follow-up of a randomised open-label trial[J]. Lancet Neurol, 2017, 16(5): 369-76. doi: 10.1016/S1474-4422(17)30047-9 [10] 雷红玉, 李烨, 牛丽梅, 等.介入放射学操作中患者的受照剂量和防护[J].中国辐射卫生, 2010, 19(2): 164, 166. [11] 冯俊, 王爱玲, 程景林, 等.不同类型心血管介入手术辐射剂量分析[J].中华放射医学与防护杂志, 2012, 32(4): 416-9. doi: 10.3760/cma.j.issn.0254-5098.2012.04.024 [12] 丁海岭, 王永春, 江薇.剂量面积乘积数据库在心血管介入职业辐射防护中的价值分析[J].中华放射医学与防护杂志, 2017, 37(8): 623- 5, 629. doi: 10.3760/cma.j.issn.0254-5098.2017.08.013 [13] Miller DL, Balter S, Cole PE, et al. Radiation doses in interventional radiology procedures: the RAD-IR study: part Ⅰ: overall measures of dose[J]. J Vasc Interv Radiol, 2003, 14(6): 711-27. doi: 10.1097/01.RVI.0000079980.80153.4B [14] 丁海岭, 张凯, 戴力赫, 等.冠状动脉造影中汉族人群体重指数与剂量面积乘积和透视时间相关性研究[J].介入放射学杂志, 2015, 24 (9): 763-6. doi: 10.3969/j.issn.1008-794X.2015.09.005 [15] Shah A, Das P, Subkovas E, et al. Radiation dose during coronary angiogram: relation to body mass index[J]. Heart Lung Circ, 2015, 24(1): 21-5. doi: 10.1016/j.hlc.2014.05.018 [16] Thijssen DH, Carter SE, Green DJ. Arterial structure and function in vascular ageing: are You as old as your arteries?[J]. J Physiol, 2016, 594(8): 2275-84. doi: 10.1113/JP270597 [17] Lapergue B, Blanc R, Gory B, et al. Effect of endovascular contact aspiration vs stent retriever on revascularization in patients with acute ischemic stroke and large vessel occlusion: the ASTER randomized clinical trial[J]. JAMA, 2017, 318(5): 443-52. doi: 10.1001/jama.2017.9644 [18] Farah J, Rouchaud A, Henry T, et al. Dose reference levels and clinical determinants in stroke neuroradiology interventions[J]. Eur Radiol, 2019, 29(2): 645-53. doi: 10.1007/s00330-018-5593-x [19] Mooney RB, McKinstry J. Paediatric dose reduction with the introduction of digital fluorography[J]. Radiat Prot Dosimetry, 2001, 94(1/2): 117-20. [20] 刘伟宾, 黄连军, 郭久芳, 等.心血管疾病患者在介入诊疗过程中辐射剂量分析[J].介入放射学杂志, 2014, 23(11): 941-4. doi: 10.3969/j.issn.1008-794X.2014.11.003 [21] 李刚, 梁保辉, 高之振, 等.介入放射学中患者的辐射剂量研究现状[J].中国辐射卫生, 2015, 24(4): 446-8. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 620
- HTML全文浏览量: 318
- PDF下载量: 3
- 被引次数: 0