



Value of ultrasound combined with X-ray on surgical treatment of patients with primary hepatolithiasis
-
摘要:
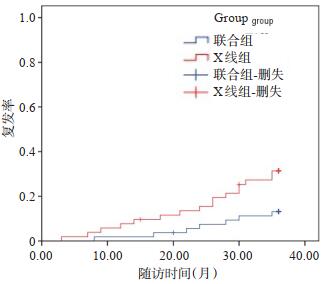
目的超声结合X线对原发性肝内胆管结石(PHL)患者经皮肝胆穿刺引流术(PTCD)治疗的指导作用和临床效果。 方法选取2017年6月~2019年6月我院114例PHL患者为研究对象,采用随机数字表法将患者分为联合组和X线组,57例/组,联合组B超结合X线引导下进行PTCD治疗,X线组仅在C臂X线透视下实施PTCD,比较两组围术期情况、治疗效果、肝功能、复发情况和并发症。 结果联合组手术时间、穿刺次数、术中出血量、胃肠蠕动恢复时间及住院时间少于X线组(P < 0.05);联合组和X线组手术成功率分别为98.15%、90.38%,差异无统计学意义(P>0.05),结石残留率分别为5.56%、19.23%,差异有统计学意义(P < 0.05);术后第3天两组血清总胆红素、谷丙转氨酶及淀粉酶水平明显升高(P < 0.05),且联合组血清总胆红素、谷丙转氨酶及淀粉酶水平低于X线组,差异有统计学意义(P < 0.05);术后3年复发率分别为12.96%、0.77%(P < 0.05);两组并发症发生率分别为14.81%、2.69%(P < 0.05)。 结论B超结合X线指导PHL患者PTCD治疗可增加定位和穿刺准确性,提升结石清除效果并减轻肝组织结构和功能损伤,减轻机体炎症反应,减少术后并发症发生。 Abstract:ObjectiveTo explore the guiding and clinical effects of ultrasound combined with X-ray on percutaneous transhepatic cholangial drainage (PTCD) in patients with primary hepatolithiasis (PHL). MethodsA total of 114 patients with PHL in our hospital from June 2017 to June 2019 were selected. They were divided into combined group and X-ray group according to the random number table method, with 57 cases in each group. Combined group was given PTCD treatment under B-ultrasound combined with X-ray guidance, and X-ray group was given PTCD only under C-shaped arm X-ray perspective.The perioperative conditions, treatment effects, liver function, recurrence and complications were compared between the two groups. ResultsThe operative time, puncture frequency, intraoperative blood loss, recovery time of gastrointestinal peristalsis and hospital stay in combined group were significantly less than those in X-ray group (P < 0.05). The success rates of surgery in combined group and X-ray group were 98.15% and 90.38% respectively (P>0.05). The residual stone rates were 5.56% and 19.23% (P < 0.05). On the 3rd day after operation, the levels of serum TBIL, ALT and amylase were significantly increased in the two groups (P < 0.05). The levels of serum TBIL, ALT and amylase in combined group were lower than those in X-ray group (P < 0.05). The recurrence rates at 3 years after operation were 12.96 % and 30.77% (P < 0.05).The incidence rates of complications in two groups were 14.81% and 32.69%, respectively (P < 0.05). ConclusionPTCD treatment guided by B-ultrasound combined with X-ray for PHL patients can improve the accuracy of localization and puncture, enhance the stone removal effects and reduce the structural and functional damage of liver tissue. It can relieve the body inflammatory response and reduce occurrence of postoperative complications. -

图 2 患者女性,46岁,超声引导PTCD
A:导丝置入; B:胆管穿刺; C:胆管扩张.
Figure 2. Ultrasound-guided PTCD, 46-year-old female patient.
表 1 两组围术期指标比较
Table 1. Comparison of perioperative indicators between the two groups (Mean±SD)
分组 手术时间(min) 穿刺次数(次) 术中出血量(mL) 胃肠蠕动恢复时间(d) 住院时间(d) 联合组(n=54) 64.39±12.58 1.45±0.26 43.61±13.02 2.13±0.48 8.71±2.04 X线组(n=52) 82.06±14.21 1.87±0.45 61.94±15.79 2.56±0.63 10.35±2.46 t 6.785 5.911 6.531 3.962 3.742 P < 0.001 < 0.001 < 0.001 < 0.001 < 0.001  下载: 导出CSV
下载: 导出CSV
表 2 两组手术效果比较
Table 2. Comparison of surgical effects between two groups[n(%)]
分组 手术成功率 结石残留率 结石复发率 联合组(n=54) 53 (98.15) 3 (5.56) 1 (1.85) X线组(n=52) 47 (90.38) 10 (19.23) 9 (13.46) χ2/Fisher - 4.604 - P 0.109 0.032 0.030
下载: 导出CSV
表 3 两组手术前后实验室指标比较
Table 3. Comparison of laboratory indicators before and after surgery between two groups (Mean±SD)
分组 TBIL (μmol/L) ALT (U/L) 淀粉酶(U/L) 术前 术后 术前 术后 术前 术后 联合组(n=54) 13.87±2.19 19.42±3.74* 26.93±4.61 32.04±6.27* 278.53±52.16 402.95±76.23* X线组(n=52) 14.25±2.36 21.60±4.58* 27.45±4.38 35.12±6.83* 280.41±51.68 435.72±79.34* t 0.860 2.689 0.595 2.42 0.186 2.169 P 0.392 0.008 0.553 0.017 0.853 0.032 *P < 0.05 vs同组术前.
下载: 导出CSV
表 4 两组术后并发症比较
Table 4. Comparison of postoperative complications between two groups[n(%)]
分组 胆管炎 胆瘘 胆道出血 急性胰腺炎 胃肠不适 合计 联合组(n=54) 1 (0) 1 (1.85) 0 (0) 2 (3.70) 4 (7.41) 8 (14.81) X线组(n=52) 3 (5.45) 2 (3.85) 3 (5.45) 4 (8.51) 5 (9.62) 17 (32.69) χ2/Fisher - - - - - 4.698 P 0.358 0.614 0.243 0.433 0.739 0.030
下载: 导出CSV
-
[1] 陈江明, 耿小平.肝内胆管结石外科治疗中的困惑[J].肝胆外科杂志, 2017, 25(3): 164-7. http://d.old.wanfangdata.com.cn/Periodical/gdwkzz201703002 [2] Plentz RR, Malek NP. Clinical presentation, risk factors and staging systems of cholangiocarcinoma[J]. Best Pract Res Clin Gastroenterol, 2015, 29(2): 245-52. https://pubmed.ncbi.nlm.nih.gov/25966425/ [3] 周毅, 胡亿龙, 袁晟光.原发性肝内胆管结石的病因及外科治疗新进展[J].肝胆胰外科杂志, 2016, 28(4): 351-3. http://d.old.wanfangdata.com.cn/Periodical/gdywkzz201604027 [4] Zang JF, Yuan Y, Zhang C, et al. Management of impacted common bile duct stones during a laparoscopic procedure: a retrospective cohort study of 377 consecutive patients [J]. Int J Surg, 2016, 32: 1-5. https://www.sciencedirect.com/science/article/pii/S1743919116301649 [5] Tsuyuguchi T, Miyakawa K, Sugiyama H, et al. Ten-year long-term results after non-surgical management of hepatolithiasis, including cases with choledochoenterostomy[J]. J Hepatobiliary Pancreat Sci, 2014, 21(11): 795-800. http://www.wanfangdata.com.cn/details/detail.do?_type=perio&id=12fd3b2179a5e92cfe19752d7c4b0211 [6] 李连举, 陈浩, 龚建平.肝胆管结石病的诊治进展[J].中国现代普通外科进展, 2018, 21(1): 64-7. http://d.old.wanfangdata.com.cn/Periodical/zwyxyj201018009 [7] Yang Q, Zhou Y, Li FY, et al. Effects of epidermal growth factor receptor inhibitor on proliferative cholangitis in hepatolithiasis[J]. HBPD Int, 2015, 14(5): 509-15. http://www.wanfangdata.com.cn/details/detail.do?_type=perio&id=gjgdybzz-z201505009 [8] Kim HJ, Kim JS, Joo MK, et al. Hepatolithiasis and intrahepatic cholangiocarcinoma: a review[J]. World J Gastroenterol, 2015, 21 (48): 13418-31. http://d.old.wanfangdata.com.cn/Periodical/syazzz201403018 [9] Okuno M, Iwashita T, Yoshida K, et al. Significance of endoscopic sphincterotomy preceding endoscopic papillary large balloon dilation in the management of bile duct stones[J]. Dig Dis Sci, 2016, 61(2): 597-602. http://www.wanfangdata.com.cn/details/detail.do?_type=perio&id=565f9133fef8d455920effadbd95e53f [10] 胡建军, 董家鸿.肝内胆管结石的外科治疗研究进展[J].中国现代普通外科进展, 2016, 19(4): 296-9. http://d.old.wanfangdata.com.cn/Periodical/zgxdptwkjz201604012 [11] Komaya K, Ebata T, Fukami Y, et al. Percutaneous biliary drainage is oncologically inferior to endoscopic drainage: a propensity score matching analysis in resectable distal cholangiocarcinoma[J]. J Gastroenterol, 2016, 51(6): 608-19. doi: 10.1007/s00535-015-1140-6 [12] 黄毅斌, 端学军, 胡萍香, 等.超声导航辅助经皮穿刺胆管置管引流术治疗肝内胆管结石梗阻效果观察[J].中华实用诊断与治疗杂志, 2016, 30(3): 287-9. http://d.old.wanfangdata.com.cn/Periodical/syzdyzlzz201603027 [13] Li X, Yu J, Liang P, et al. Ultrasound-guided percutaneous microwave ablation assisted by three-dimensional visualization operative treatment planning system and percutaneous transhepatic cholangial drainage with intraductal chilled saline perfusion for larger hepatic hilum hepatocellular (D≥3 cm): preliminary results[J]. Oncotarget, 2017, 8(45): 79742-9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5668087/ [14] 蔡丽萍, 朱霞, 成亚芹, 等.超声造影在胆道阻塞性疾病超声引导置管引流术中的应用价值[J].临床超声医学杂志, 2014, 16(9): 606-9. http://d.old.wanfangdata.com.cn/Periodical/lccsyxzz201409011 [15] 庄晓惠, 许春芳.抗B7-H3单克隆抗体抑制雨蛙肽诱导的小鼠急性胰腺炎炎症反应和组织损伤[J].细胞与分子免疫学杂志, 2016, 32(3): 323-7. http://d.old.wanfangdata.com.cn/Periodical/xbyfzmyxzz201603008 [16] Park JS, Jeong S, Lee DH, et al. Risk factors for long-term outcomes after initial treatment in hepatolithiasis[J]. J Korean Med Sci, 2013, 28(11): 1627-31. http://d.old.wanfangdata.com.cn/OAPaper/oai_pubmedcentral.nih.gov_3835505 [17] 彭朝阳.肝叶切除术治疗后肝内胆管结石复发的危险因素研究[J].中国全科医学, 2017, 38(A01): 163-5. http://www.cnki.com.cn/Article/CJFDTotal-QKYX2017S1060.htm [18] 廖伟明, 温钦, 吴振声, 等. B超定位联合X线引导经皮经肝穿刺碎石取石术治疗肝内胆管结石[J].中国普通外科杂志, 2016, 25(8): 1117-22. http://d.old.wanfangdata.com.cn/Periodical/zgptwkzz201608006 [19] 李云, 谢升华.超声引导下经皮肝穿刺胆管造瘘电子胆道镜取石术对肝内胆管结石患者并发症的影响分析[J].中国医药科学, 2019, 9 (16): 249-51. http://d.old.wanfangdata.com.cn/Periodical/zgyykx201916071 [20] 李志, 张剑权, 符国珍, 等.超声引导经皮经肝一期胆道镜碎石取石术治疗肝内胆管结石[J].中华肝胆外科杂志, 2018, 24(3): 208-10. http://d.old.wanfangdata.com.cn/Periodical/zhgdwk201803017 -


 点击查看大图
点击查看大图
计量
- 文章访问数: 652
- HTML全文浏览量: 346
- PDF下载量: 5
- 被引次数: 0