



Diagnosis and treatment of syphilitic myelitis confirmed by pathology: 2 cases report and literature review
-
摘要:
目的 探讨梅毒性脊髓炎的诊断及治疗。 方法 报告我科行手术治疗、病理确诊的2例梅毒性脊髓炎患者的临床特征、影像学资料、病理学表现和治疗方法,并结合相关文献复习,对上述资料进行分析总结。 结果 病例1:47岁女性患者,腰骶部疼痛2年余,血清学示梅毒(+),行后路胸椎穿刺活检术,考虑诊断T12肿瘤,后行后路胸12椎体病灶清除,取自体髂骨椎间植骨融合内固定术,术中病理提示符合梅毒树胶肿改变。病例2:34岁男性患者,诊断三期梅毒1年余,腰痛伴跛行2月余,行腰椎穿刺活检术,提示L5/S1梅毒性脊柱炎合并脊柱结核。行后路椎管减压、病灶清除、椎间盘摘除、椎间植骨融合内固定术。2例患者术前、术后均行苄星青霉素抗梅毒治疗,术后症状较前明显好转、复查指标下降、影像学资料提示病灶缩小。 结论 梅毒性脊柱炎临床上极为罕见,明确诊断后经过全身性的抗梅毒治疗、手术治疗,病灶缩小、症状好转,有较好的预后及疗效。 Abstract:Objective To analyze the diagnosis and treatment of syphilitic myelitis. Methods The clinical features, imaging data, pathological manifestations and treatment of 2 patients with syphilitic myelitis diagnosed by operation and pathology in our department were reported. The clinical data were analyzed and summarized combined with the review of related literature. Results Case 1: a 47-year-old female patient with lumbosacral pain for more than 2 years. The serology showed syphilis (+) and posterior thoracic puncture biopsy was performed. T12 tumor was diagnosed, and posterior debridement of T12 vertebrae was performed. Autogenous iliac bone graft fusion and internal fixation was performed. The pathological findings were consistent with the changes of syphilis. Case 2: a 34-year-old male patient was diagnosed with tertiary syphilis for more than 1 year and low back pain with lameness for more than 2 months. Lumbar puncture biopsy showed that L5/S1 syphilis spondylitis complicated with spinal tuberculosis. Posterior spinal canal decompression, focus debridement, discectomy, interbody fusion and internal fixation were performed. Two patients were treated with benzylpenicillin anti-syphilis before and after operation. The postoperative symptoms were significantly improved, the reexamination index decreased, and the imaging data indicated that the focus was reduced. Conclusions Syphilitic spondylitis is extremely rare in clinic. After systemic antisyphilis treatment and surgical treatment, the focus is reduced and the symptoms are improved, which has a good prognosis and curative effect. -
Key words:
- syphilis /
- spinal infection /
- pathological examination /
- imaging examination
-

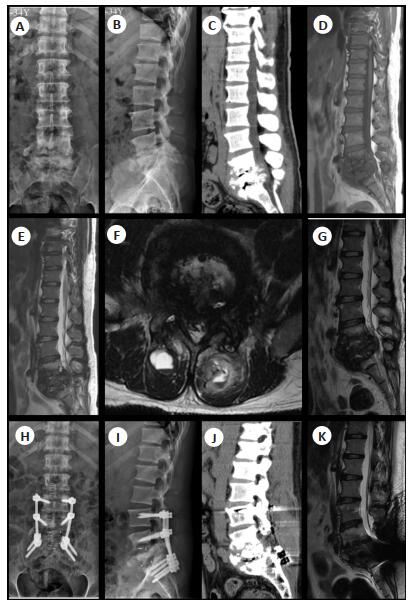
图 1 病例1影像学表现
患者47岁女性, 诊断为T12梅毒性脊髓炎; A-B:术前X线、CT提示T12椎体压缩、骨质破坏(如箭头所示), C-F:脊柱MRI提示T12椎体楔形变(如箭头所示), 相应椎管狭窄, 可见软组织影.增强MRI(F)示椎体及其附件明显强化, G-H:行后路T12椎体全切、椎管减压、椎间植骨融合内固定术后, 复查X线提示内固定位置良好.
Figure 1. Imaging findings of case 1.

图 2 病例1术中资料
行后路胸12椎体病灶清除、椎间植骨融合内固定术, 术中以胸12棘突为中心作后正中切口, 长约28 cm; 逐层切开皮肤、皮下组织, 沿棘突切开腰背筋膜及骶棘肌, 安放椎板自动撑开器撑开固定, 显露胸9-腰3棘突、椎板及上下小关节突; 可见胸12两侧椎板破坏, 以右侧明显并形成包膜, 用髓核钳取出右侧大块病灶样组织送术中冰冻切片病理学检查.
Figure 2. Intraoperative data of case 1.

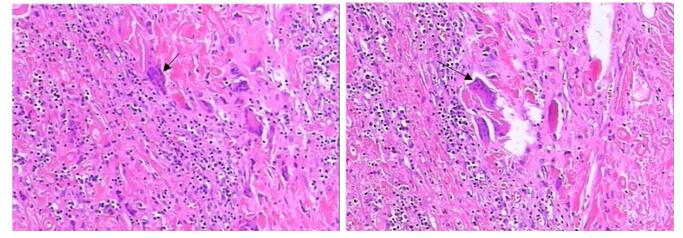
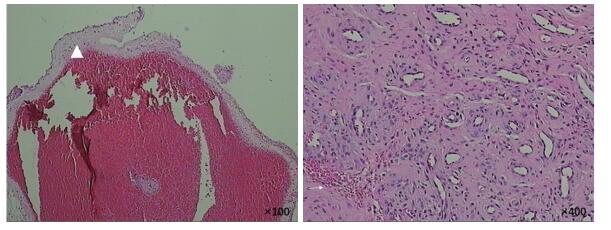
图 3 病例1病理学资料
手术取病理标本可见多个由类上皮细胞和多核巨细胞组成的结节(如箭头所示), 符合梅毒树胶肿改变.
Figure 3. Pathological data of Case 1 (HE, ×400).

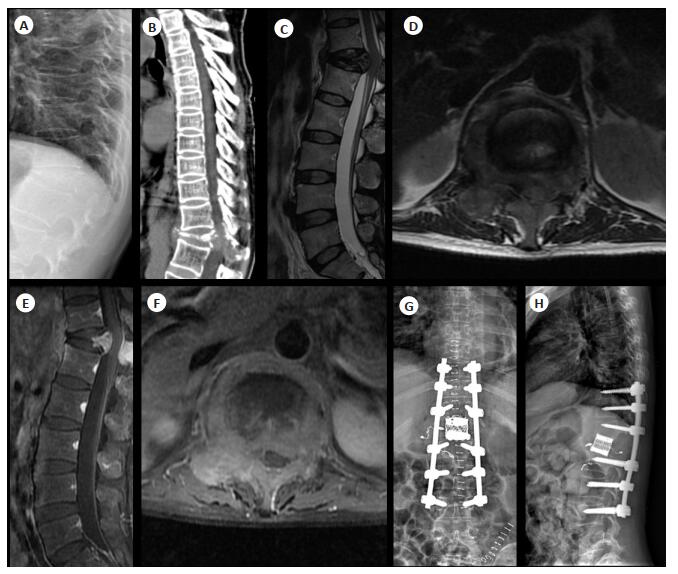
图 4 病例2影像学资料
35岁男性, 既往有2年三期梅毒病史; A-C:术前X线和CT提示骨质破坏(如箭头所示)和脓肿形成(L4-S1); D-G:脊柱MRI(2017年1月17日)发现L4-S1椎体“虫蚀样”骨质破坏(如箭头所示), L4-S1椎间盘严重破坏, 相应节段椎管严重狭窄, 双侧竖脊肌可见异常信号(如三角形所示); H-I:经后路L4-S1椎管减压、椎间植骨融合内固定术后复查X线提示内固定位置良好; J-K:术后6月复查CT、MRI提示病灶较前明显缩小, 脓肿消失.
Figure 4. Imaging findings of case 2.
-
[1] Fenton KA, Breban R, Vardavas R, et al. Infectious syphilis in high-income settings in the 21st century[J]. Lancet Infect Dis, 2008, 8(4): 244-53. https://pubmed.ncbi.nlm.nih.gov/18353265/ [2] Conde-Sendín MA, Amela-Peris R, Aladro-Benito Y, et al. Current clinical spectrum of neurosyphilis in immunocompetent patients[J]. Eur Neurol, 2004, 52(1): 29-35. doi: 10.1159/000079391 [3] Chilver-Stainer L, Fischer U, Hauf M, et al. Syphilitic myelitis: rare, nonspecific, but treatable[J]. Neurology, 2009, 72(7): 673-5. doi: 10.1212/01.wnl.0000342460.07764.5c [4] Joob B, Wiwanitkit V. Clinical spectrum of neurosyphilis in north east India[J]. Neurol India, 2011, 59(5): 794-5. doi: 10.4103/0028-3886.86587 [5] Tsui EY, Ng SH, Chow L, et al. Syphilitic myelitis with diffuse spinal cord abnormality on MR imaging[J]. Eur Radiol, 2002, 12(12): 2973-6. doi: 10.1007/s00330-001-1244-7 [6] Timmermans M, Carr J. Neurosyphilis in the modern era[J]. J Neurol Neurosurg Psychiatry, 2004, 75(12): 1727-30. doi: 10.1136/jnnp.2004.031922 [7] Simon RP. Neurosyphilis[J]. West J Med, 1988, 149(1): 80-1. http://d.old.wanfangdata.com.cn/Periodical/lcsjbxzz200302011 [8] Chilver-Stainer L, Fischer U, Hauf M, et al. Syphilitic myelitis: rare, nonspecific, but treatable[J]. Neurology, 2009, 72(7): 673-5. doi: 10.1212/01.wnl.0000342460.07764.5c [9] Tashiro K, Moriwaka F, Sudo K, et al. Syphilitic myelitis with its magnetic resonance imaging (MRI) verification and successful treatment[J]. Jpn J Psychiatry Neurol, 1987, 41(2): 269-71. https://www.deepdyve.com/lp/wiley/syphilitic-myelitis-with-its-magnetic-resonance-imaging-mri-4R3Dt2b4xX [10] Kikuchi S, Shinpo K, Niino M, et al. Subacute syphilitic meningomyelitis with characteristic spinal MRI findings[J]. J Neurol, 2003, 250(1): 106-7. doi: 10.1007-s00415-003-0921-7/ [11] Nesbit GM, Miller GM, Baker HL Jr, et al. Spinal cord sarcoidosis: a new finding at MR imaging with Gd-DTPA enhancement[J]. Radiology, 1989, 173(3): 839-43. doi: 10.1148/radiology.173.3.2813795 [12] Gupta R, Garg RK, Jain A, et al. Spinal cord and spinal nerve root involvement (myeloradiculopathy) in tuberculous meningitis[J]. Medicine, 2015, 94(3): e404-12. https://www.ncbi.nlm.nih.gov/pubmed/25621686 [13] Kararizou E, Anagnostou E, Kapaki E, et al. Chronic inflammatory demyelinating polyneuropathy associated with neurosyphilis[J]. Am J Med Sci, 2015, 349(1): 90-1. doi: 10.1097/MAJ.0000000000000369 [14] Marra CM. Syphilis screening in neurology[J]. J Am Med Assco Neurol, 2016, 73(8): 926-7. doi: 10.1001/jamaneurol.2016.1955 [15] Kingston M, French P, Higgins S, et al. UK national guidelines on the management of syphilis 2015[J]. Int J STD AIDS, 2016, 27(6): 421-46. doi: 10.1177/0956462415624059 [16] Workowski KA. Centers for Disease Control and Prevention Sexually Transmitted Diseases Treatment Guidelines[J]. MMWR Recomm Rep, 2015, 64(RR-03): 1-137. doi: 10.1086-511421/ [17] Yang CL, Li G, Fang JY, et al. Spinal intramedullary syphilitic gumma: an unusual presentation of neurosyphilis [J]. World Neurosurg, 2016, 95: 622-9. http://www.ncbi.nlm.nih.gov/pubmed/27452967 [18] Griffiths RW, Rose MJ. Acute vertebral collapse and cauda equina compression in tertiary syphilis[J]. J Neurol Neurosurg Psychiatry, 1975, 38(6): 558-60. https://www.ncbi.nlm.nih.gov/pubmed/1151423 [19] Yin R, Wang L, Zhang T, et al. Syphilis of the lumbar spine: A case report and review of the literature[J]. Medicine, 2017, 96(50): e9098-103. doi: 10.1097/MD.0000000000009098 -

 下载:
下载:

 点击查看大图
点击查看大图
计量
- 文章访问数: 999
- HTML全文浏览量: 411
- PDF下载量: 11
- 被引次数: 0