



Value of real-time shear wave elastography in evaluating the damage in chronic kidney disease
-
摘要:
目的 探讨实时剪切波弹性成像(RT-SWE)技术在慢性肾脏疾病早期肾损害中的潜在应用价值。 方法 应用RT-SWE技术检测早期慢性肾病1~3期患者肾脏皮质杨氏模量均值(Emean),与患者24 h尿蛋白定量、血肌酐值及肾穿刺活检病理间质纤维化程度作对比;引入年龄因素校正Emean值(pyEmean),比较早期慢性肾病各期患者pyEmean值的差异。 结果 Emean值在慢性肾病1~3期患者不同组的差异无统计学意义(P > 0.05);根据患者年龄校正得出的pyEmean值在慢性肾病1期与2期患者之间差异无统计学意义(P > 0.05),但1、2期与3期的差异有统计学意义(P < 0.05)。 结论 pyEmean值排除了年龄对肾脏硬度值的影响,对评估早期慢性肾病患者肾脏纤维化程度可能具有重要的潜在应用价值,RT-SWE技术可以应用于慢性肾病早期肾损害评估。 Abstract:Objective To investigate the value of RT-SWE technology in early damage of chronic kidney disease. Methods Emean modulus of renal cortex in patients with chronic kidney disease (stage 1-3) was detected by RT-SWE technique, which was compared with 24-hour urinary protein quantification, serum creatinine value and interstitial fibrosis degree in with renal biopsy. Age factor was introduced to adjust the Emean value (pyEmean). The differences of pyEmean value in patients with early chronic kidney disease at all stages were compared. Results The difference in Emean value between the groups of patients with chronic kidney disease stage 1-3 was not significant (P > 0.05).The difference in pyEmean value obtained by age correction between stage 1 and stage 2 chronic kidney disease patients was not significant (P > 0.05). The difference between stage 1, 2 and 3 was significant (P < 0.05). Conclusions pyEmean excludes the influence of age on renal hardness. It has important potential application value in the evaluation of renal fibrosis in early chronic kidney disease patients. RT-SWE technology can be used in the evaluation of early renal damage in chronic kidney disease. -

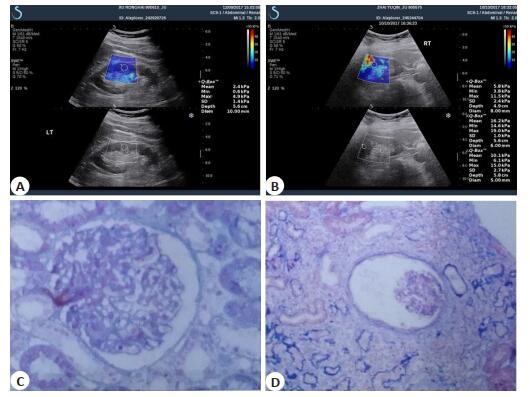
图 2 RT-SWE图像与肾穿刺活检电镜图像示例
A: CKD 1期患者肾脏弹性图像; B: CKD 3期患者肾脏弹性图像; C:患者(A)电镜MASSON染色显示其肾间质无明显纤维化; D:患者(B)电镜MASSON染色显示其肾间质纤维化 < 15%.
Figure 2. Typical example of RT- SWE image and electron microscopy of renal biopsy image.

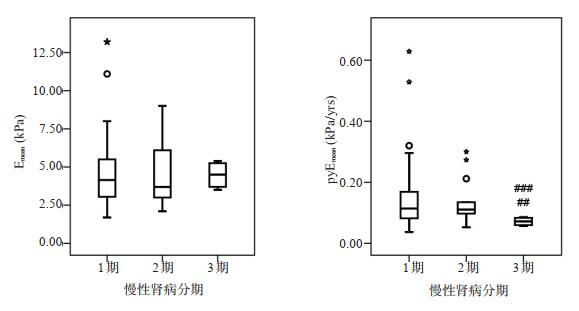
图 3 CKD1~3期组间Emean及pyEmean的组间比较
Figure 3. Comparison of Emean and pyEmean between groups in stage 1-3 of chronic kidney disease.
表 1 早期CKD患者分期情况
Table 1. Grouping of early chronic kidney disease patients
CKD分期 肾小球滤过率[mL/(min·1.73 m2)] 1期 GFR正常, GFR≥90但已有肾损害(蛋白尿、血尿) 2期 GFR轻度下降, 伴肾脏损害, 60≤GFR < 90 3期 GFR中度下降, 30≤GFR < 60 CKD: Chronic kidney disease.  下载: 导出CSV
下载: 导出CSV
表 2 患者一般资料对比
Table 2. Comparison of general information of patients in three stages
指标 CKD 1期(n=32) CKD 2期(n=14) CKD 3期(n=9) 总计(n=55) 年龄(岁, Mean±SD) 36.6±14.1 38.0±14.6 62.5±0.6*# 39.1±15.2 男性[n(%)] 14 (43.8) 6 (42.9) 4 (44.4) 24 (43.6) 24 hUT (g/24 h, Mean±SD) 4.4±5.6 5.8±2.9* 2.2±2.2# 4.6±4.8 SCr (μmmol/L, Mean±SD) 69.4±14.4 92.8±12.7* 145.7±61.9* 82.1±29.6 间质纤维化程度(%) 0.94±0.76 1.14±0.36 1.50±0.58 1.04±0.67a Emean (kPa, Mean±SD) 4.7±2.5 4.7±2.2 4.5±0.9 4.7±2.3 *P < 0.05 vs CKD 1期; #P < 0.05 vs CKD 2期; 采用整体卡方检验比较, P=0.967; a采用整体卡方检验比较, P=0.033.
下载: 导出CSV
表 3 患者Emean值及pyEmean值对比
Table 3. Comparison of Emean value and pyEmean value of patients in three stages
指标 CKD 1期(n=32) CKD 2期(n=14) CKD 3期(n=9) 总计(n=55) 年龄(岁, Mean±SD) 36.6±14.1 38.0±14.6 62.5±0.6*# 39.1±15.2 男性[n(%)] 14 (43.8) 6 (42.9) 4 (44.4) 24 (43.6%) Emean值(kPa, Mean±SD) 4.7±2.5 4.7±2.2 4.5±0.9 4.7±2.3 pyEmean值(kPa/岁, Mean±SD) 0.16±0.13 0.13±0.07 0.07±0.01*# 0.14±0.11 *P < 0.05 vs CKD 1期; #P < 0.05 vs CKD 2期; 采用整体卡方检验比较, P=0.967.
下载: 导出CSV
-
[1] National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification [J]. Am J Kidney Dis, 2002, 39(2 Suppl 1): S1-S266. https://pubmed.ncbi.nlm.nih.gov/11904577/ [2] Muntner P, Judd SE, McClellan W, et al. Incidence of stroke symptoms among adults with chronic kidney disease: results from the REasons for Geographic And Racial Differences in Stroke (REGARDS) study[J]. Nephrol Dial Transplant, 2012, 27(1): 166-73. doi: 10.1093/ndt/gfr218 [3] Carrol LE. The stages of chronic kidney disease and the estimated glomerular filtration rate[J]. J Lancaster Gen Hosp, 2006, 1: 64-9 http://d.old.wanfangdata.com.cn/OAPaper/oai_doaj-articles_e2d9b0f21c21ad46c244aaef5cf65c3a [4] Blaser R, Provenzano R. The medicare quality improvement act in program and abstracts of the kidney disease economics conference [M]. Phoenix: Arizona, 2005. [5] Cui GH, Yang Z, Zhang WX, et al. Evaluation of acoustic radiation force impulse imaging for the clinicopathological typing of renal fibrosis[J]. Exp Ther Med, 2014, 7(1): 233-5. doi: 10.3892/etm.2013.1377 [6] Gya C, Hamidi C, Ece A, et al. Acoustic radiation force impulse (ARFI) elastography for detection of renal damage in children[J]. Pediatr Radiol, 2015, 45(1):55-61. http://www.wanfangdata.com.cn/details/detail.do?_type=perio&id=534ab0c10a8709ae008fa7e92fb47253 [7] Bota S, Bob F, Sporea I, et al. Factors that influence kidney shear wave speed assessed by acoustic radiation force impulse elastography in patients without kidney pathology[J]. Ultrasound Med Biol, 2015, 41(1): 1-6. https://www.ncbi.nlm.nih.gov/pubmed/25438855 [8] Menzilcioglu MS, Duymus M, Citil S, et al. Strain wave elastography for evaluation of renal parenchyma in chronic kidney disease[J]. Br J Radiol, 2015, 88(1050): 20140714. doi: 10.1259/bjr.20140714 [9] 齐向明.钙神经蛋白抑制剂对糖尿病肾脏炎症的调节作用及其机制研究[D].合肥: 安徽医科大学, 2013. http://cdmd.cnki.com.cn/Article/CDMD-10366-1013337343.htm [10] 金惠铭, 王建枝.病理生理学[M].北京:人民卫生出版社, 2008: 258- 63. [11] Sporea I, Bota S, Gradinaru-Taşcău O, et al. Which are the cut-off values of 2D-Shear Wave Elastography (2D-SWE) liver stiffness measurements predicting different stages of liver fibrosis, considering Transient Elastography (TE) as the reference method[J]. Eur J Radiol, 2014, 83(3): e118-22. https://www.sciencedirect.com/science/article/pii/S0720048X13006542 [12] Grenier N, Poulain S, Lepreux S, et al. Quantitative elastography of renal transplants using supersonic shear imaging: a pilot study[J]. Eur Radiol, 2012, 22(10): 2138-46. doi: 10.1007/s00330-012-2471-9 [13] Bob F, Bota S, Sporea I, et al. Kidney shear wave speed values in subjects with and without renal pathology and inter-operator reproducibility of acoustic radiation force impulse elastography (ARFI): preliminary results[J]. PLoS One, 2014, 9(11): e113761. doi: 10.1371/journal.pone.0113761 [14] Guo LH, Xu HX, Fu HJ, et al. Acoustic radiation force impulse imaging for noninvasive evaluation of renal parenchyma elasticity: preliminary findings[J]. PLoS One, 2013, 8(7): e68925-9. doi: 10.1371/journal.pone.0068925 [15] Dai X, Liu MH, Guo Y, et al. Noninvasive evaluation of renal allograft fibrosis by virtual touch tissues quantification[J]. J Central South Univ Med Sci, 2014, 39(2): 173-7. http://www.wanfangdata.com.cn/details/detail.do?_type=perio&id=hnykdx201402011 [16] Syversveen T, Brabrand K, Midtvedt K, et al. Assessment of renal allograft fibrosis by acoustic radiation force impulse quantification: a pilot study[J]. Transpl Int, 2011, 24(1):100-5. doi: 10.1111-j.1432-2277.2010.01165.x/ [17] Syversveen T, Midtvedt K, Berstad AE, et al. Tissue elasticity estimated by acoustic radiation force impulse quantification depends on the applied transducer force: an experimental study in kidney transplant patients[J]. Eur Radiol, 2012, 22(10):2130-7. doi: 10.1007/s00330-012-2476-4 [18] Lee J, Oh YT, Joo DJ, et al. Acoustic radiation force impulse measurement in renal transplantation: a prospective, longitudinal study with protocol biopsies[J]. Medicine (Baltimore), 2015, 94(39): e1590. doi: 10.1097/MD.0000000000001590 [19] Bob F, Grosu I, Sporea I, et al. Ultrasound-based shear wave elastography in the assessment of patients with diabetic kidney disease[J]. Ultrasound Med Biol, 2017, 43(10): 2159-66. http://www.wanfangdata.com.cn/details/detail.do?_type=perio&id=4445ae1f37c46405d0f53f1e5b767385 [20] Tian F, Wang ZB, Meng DM, et al. Preliminary study on the role of virtual touch tissue quantification combined with a urinary β2-microglobulin test on the early diagnosis of gouty kidney damage [J]. Ultrasound Med Biol, 2014, 40(7): 1394-9. doi: 10.1016/j.ultrasmedbio.2014.01.013 -

 点击查看大图
点击查看大图

计量
- 文章访问数: 690
- HTML全文浏览量: 274
- PDF下载量: 4
- 被引次数: 0