



Efficacy of bilateral internal mammary arterial grafting for elderly diabetic patients and imaging follow-up
-
摘要:
目的 探讨老年(60~75岁)糖尿病患者接受双侧乳内动脉(BIMA)搭桥手术的早期(3月)疗效及影像学随访结果,总结针对该类患者的诊疗经验。 方法 回顾性分析2015年12月~2017年8月于我科接受BIMA搭桥术的64例老年患者,将其按是否患有糖尿病分为糖尿病组和非糖尿病组。糖尿病组36例,男性25例,女性11例,年龄62.83±2.60岁;非糖尿病组28例,男性23例,女性5例,年龄62.29±1.76岁。分析两组患者术前一般情况、术中资料(主动脉阻断时间、体外循环时间、手术时间等)、术后常见并发症的发生率、影像学随访结果等资料,探讨该类患者的早期手术疗效,总结诊疗经验。 结果 糖尿病组“左主干+三只血管病变”的患病率及术前糖化血红蛋白水平均高于非糖尿病组(P=0.025、0.001)。两组患者在骨骼化获取乳内动脉例数、手术时间、体外循环时间、主动脉阻断时间、乳内动脉桥的即刻血流量及搏动指数(PI值)等方面差异无统计学意义(P > 0.05)。两组患者胸部切口愈合不良、乳糜胸等常见并发症的发生率差异无统计学意义(P > 0.05);4例患者合并术后胸部切口并发症,其术前的糖化血红蛋白水平高于其他患者(P < 0.001)。冠脉CT血管造影结果显示,两组患者术后早期桥血管的闭塞率差异无统计学意义(P > 0.05)。 结论 相较于非糖尿病的老年患者而言,老年糖尿病患者的冠脉病变较重,但BIMA搭桥术的手术难度无增加,在适当治疗的基础上可获得满意的早期疗效,冠脉CTA作为该类患者早期的随访方法结果较满意。 Abstract:Objective To explore the short-term (3 months) results of bilateral internal mammary artery (BIMA) grafting in elderly diabetic patients (60-75 years old). Methods From December 2015 to August 2017, 64 elderly patients who underwent BIMA grafting in our department were enrolled. They were divided into two groups: diabetic group and non-diabetic group. The diabetic group had 36 cases, including 25 males, 11 females, with an average age of 62.83±2.60 years old. Non-diabetic group had 28 cases, including 23 males and 5 females, with an average age of 62.29±1.76 years old. The clinical records, intra-operative data (aortic clamp time, cardiopulmonary bypass time, operation time, etc.), short-term complications, and imaging follow-up data of these patients were retrospectively analyzed. Results The incidence rate of left main + triple-vessel disease and preoperative HbA1c level of diabetic group were higher than those of non-diabetic group (P=0.025, 0.001). The differences of the internal mammary artery harvest technique, operation time, aortic clamp time, cardiopulmonary bypass time as well as the flow and pulsatility index of internal mammary artery grafts between two groups were not significant (P > 0.05). The difference of sternal wound complications and other common complications between these groups was not significant (P > 0.05). Four patients suffered sternal wound complications. The preoperative HbA1c level of them was significantly higher than the other's (P < 0.001). The difference of grafts occlusion between two groups was not significant (P > 0.05), according to the results of coronary CTA three months after operation. Conclusions Compared with the elderly patients without diabetes mellitus, the coronary artery lesions in the elderly (60-75 years old) diabetic patients are more serious. However, the difficulty of BIMA grafting for them are not increased. Satisfactory short-term results could be achieved on the basis of appropriate treatment. Coronary CTA as a follow-up method for these patients achieves satisfactory results. -

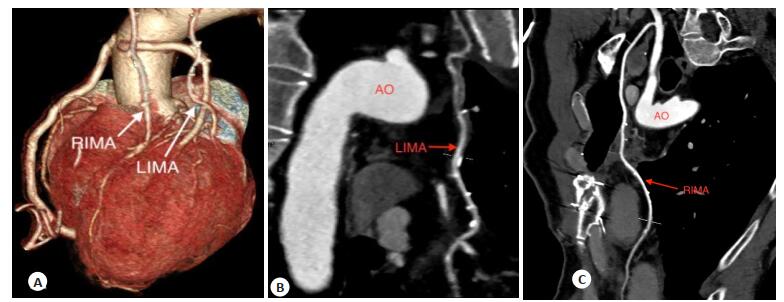
图 1 骨骼化游离双侧乳内动脉
RIMA: Right internal mammary artery; LIMA: Left internal mammary artery.
Figure 1. Bilateral internal mammary arteries harvested with skeletonization technique.

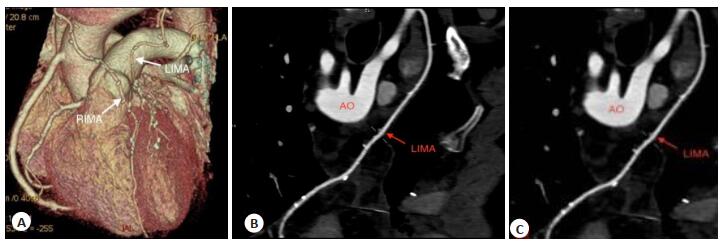
图 2 术后1月冠脉CTA结果
RIMA: Right internal mammary artery; LIMA: Left internal mammary artery; AO: Aorta.
Figure 2. Coronary CTA results at one month after operation.

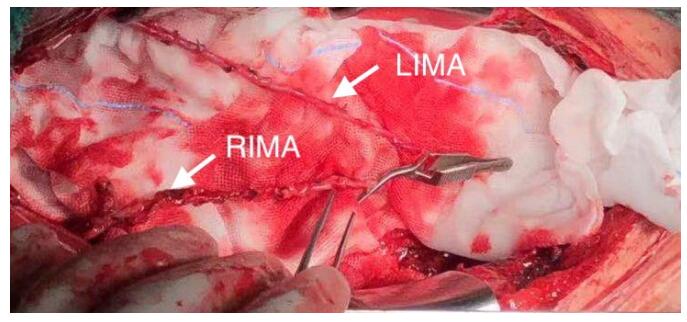
图 3 术后3月冠脉CTA结果
RIMA: Right internal mammary artery; LIMA: Left internal mammary artery; AO: Aorta.
Figure 3. Coronary CTA results at three months after operation.
表 1 两组术前一般情况
Table 1. Preoperative characteristics of two groups (Mean±SD)
指标 糖尿病组(n=36) 非糖尿病组(n=28) t/χ2 P 年龄(岁) 62.83±2.60 62.29±1.76 0.956 0.343 身高(cm) 167.19±6.84 169.25±5.33 -1.310 0.195 体质量(kg) 72.82±9.59 73.34±10.32 0.208 0.836 性别(n) 1.354 0.244 男性 25 23 女性 11 5 BMI (kg/m2) 26.01±2.65 25.52±2.73 0.730 0.468 既往病史(n) 心肌梗死 11 8 0.030 0.863 高血压 23 16 0.301 0.583 高血脂 18 16 0.323 0.570 外周动脉狭窄 16 7 2.587 0.108 术前HbA1c (%) 7.06±1.26 6.03±0.89 3.671 0.001 冠脉病变情况(%) 5.006 0.025 左主干+三支血管病变 63.89 35.71 三支血管病变 36.11 64.29 术前心功能NYHA分级(n) 0.657 0.514 Ⅰ 4 5 Ⅱ 26 19 Ⅲ 6 4 LVEDD (mm) 48.03±6.14 48.96±5.20 -0.646 0.520 LVEF (%) 60.25±8.08 62.36±5.99 -1.155 0.253 NYHA: New York Heart Disease Assocation; LVEDD: Left ventricular end-diastolic dimension; LV EF: Left ventricular ejection fraction.  下载: 导出CSV
下载: 导出CSV
表 2 两组术中资料
Table 2. Intra-operative data of the study population of two groups (Mean±SD)
指标 糖尿病组(n=36) 非糖尿病组(n=28) t/χ2 P 骨骼化获取乳内动脉(n) 26 17 0.946 0.331 手术时间(h) 4.81±0.44 4.69±0.44 1.095 0.278 体外循环时间(min) 113.92±20.45 107.43±29.57 1.037 0.304 主动脉阻断时间(min) 85.11±15.16 79.00±24.06 1.241 0.219 左乳内动脉 流量(mL/min) 27.11±13.33 27.57±9.03 -0.157 0.876 PI 2.26±0.62 2.09±0.31 1.303 0.197 右乳内动脉 流量(mL/min) 33.17±20.30 24.84±10.80 1.959 0.055 PI 2.05±0.47 2.25±0.55 -1.517 0.134 PI: Pulsatility index.
下载: 导出CSV
表 3 两组术后早期资料
Table 3. Short-term complications of the study population of two groups (n)
指标 糖尿病组(n=36) 非糖尿病组(n=28) t/χ2 P 再次开胸止血 0 0 死亡 0 0 乳糜胸 4 1 1.243 0.265 胸部伤口并发症 轻度 2 1 0.139 0.709 重度 0 1 1.306 0.253
下载: 导出CSV
表 4 两组术后3月影像随访资料
Table 4. Imaging follow up data of 3 months post-operation of two groups (%)
桥血管闭塞率 糖尿病组(n=36) 非糖尿病组(n=28) t/χ2 P 静脉桥 7.41 3.13 1.258 0.262 动脉桥 4.17 5.36 0.100 0.752
下载: 导出CSV
-
[1] Dorman MJ, Kurlansky PA, Traad EA, et al. Bilateral internal mammary artery grafting enhances survival in diabetic patients: a 30-year follow-up of propensity score-matched cohorts [J]. Circulation, 2012, 126(25): 2935-42. doi: 10.1161/CIRCULATIONAHA.112.117606 [2] Gansera B, Delalic A, Eszlari E, et al. 14-year results of bilateral versus single internal thoracic artery grafts for left-sided myocardial revascularization in young diabetic patients[J]. Thorac Cardiovasc Surg, 2017, 65(4): 272-7. http://www.ncbi.nlm.nih.gov/pubmed/27855470 [3] Itagaki S, Cavallaro P, Adams DH, et al. Bilateral internal mammary artery grafts, mortality and morbidity: an analysis of 1526360 coronary bypass operations[J]. Heart, 2013, 99(12): 849-53. doi: 10.1136/heartjnl-2013-303672 [4] Pettinari M, Sergeant P, Meuris B. Bilateral internal thoracic artery grafting increases long-term survival in elderly patients[J]. Eur J Cardiothorac Surg, 2015, 47(4): 703-9. doi: 10.1093/ejcts/ezu206 [5] 畅怡, 王小啟, 郑哲, 等.使用双侧乳内动脉行冠状动脉旁路移植术动脉桥即时流量的初步研究[J].中国循环杂志, 2017, 32(11): 1080-4. doi: 10.3969/j.issn.1000-3614.2017.11.009 [6] Itoh S, Kimura N, Adachi H, et al. Is bilateral internal mammary arterial grafting beneficial for patients aged 75 years or older[J]. Circulation, 2016, 80(8): 1756-63. http://d.old.wanfangdata.com.cn/Periodical/zgrkx201711008 [7] Locker C, Schaff HV, Dearani JA, et al. Multiple arterial grafts improve late survival of patients undergoing coronary artery bypass graft surgery: analysis of 8622 patients with multivessel disease[J]. Circulation, 2012, 126(9): 1023-30. https://pubmed.ncbi.nlm.nih.gov/22811577/ [8] Kelly R, Buth KJ, Légaré JF. Bilateral internal thoracic artery grafting is superior to other forms of multiple arterial grafting in providing survival benefit after coronary bypass surgery[J]. J Thorac Cardiovasc Surg, 2012, 144(6): 1408-15. doi: 10.1016/j.jtcvs.2012.01.030 [9] Shi WY, Hayward PA, Tatoulis J, et al. Are all forms of total arterial revascularization equal? A comparison of single versus bilateral internal thoracic artery grafting strategies[J]. J Thorac Cardiovasc Surg, 2015, 150(6): 1526-33. doi: 10.1016/j.jtcvs.2015.05.074 [10] Buxton BF, Shi WY, Tatoulis J, et al. Total arterial revascularization with internal thoracic and radial artery grafts in triple-vessel coronary artery disease is associated with improved survival[J]. J Thorac Cardiovasc Surg, 2014, 148(4): 1238-43. https://www.ncbi.nlm.nih.gov/pubmed/25131165 [11] Dimitrova KR, Hoffman DM, Geller CM, et al. Arterial grafts protect the native coronary vessels from atherosclerotic disease progression [J]. Ann Thorac Surg, 2012, 94(2): 475-81. doi: 10.1016/j.athoracsur.2012.04.035 [12] Kieser TM, Lewin AM, Graham MM, et al. Outcomes associated with bilateral internal thoracic artery grafting: the importance of age [J]. Ann Thorac Surg, 2011, 92(4): 1269-76. doi: 10.1016/j.athoracsur.2011.05.083 [13] Gatti G, Dell'Angela L, Benussi B, et al. Bilateral internal thoracic artery grafting in octogenarians: where are the benefits[J]. Heart Vessels, 2016, 31(5): 702-12. doi: 10.1007/s00380-015-0675-z [14] Rubino AS, Gatti G, Reichart D, et al. Early outcome of bilateral versus single internal mammary artery grafting in the elderly[J]. Ann Thorac Surg, 2018, 105(6): 1717-23. doi: 10.1016/j.athoracsur.2017.11.079 [15] Mohammadi S, Dagenais F, Voisine P, et al. Lessons learned from the use of 1, 977 in situ bilateral internal mammary arteries: a retrospective study[J]. J Cardiothorac Surg, 2014, 9: 158-67. doi: 10.1186/s13019-014-0158-9 [16] Gatti G, Perrotti A, Reichart D, et al. Glycated hemoglobin and risk of sternal wound infection after isolated coronary surgery[J]. Circ J, 2016, 81(1): 36-43. https://www.ncbi.nlm.nih.gov/pubmed/27928145 [17] Rollins KE, Varadhan KK, Dhatariya K, et al. Systematic review of the impact of HbA1c on outcomes following surgery in patients with diabetes mellitus[J]. Clin Nutr, 2016, 35(2): 308-16. https://www.ncbi.nlm.nih.gov/pubmed/25840840 [18] Benedetto U, Altman DG, Gerry S, et al. Pedicled and skeletonized single and bilateral internal thoracic artery grafts and the incidence of sternal wound complications: Insights from the Arterial Revascularization Trial[J]. J Thorac Cardiovasc Surg, 2016, 152(1): 270-6. doi: 10.1016/j.jtcvs.2016.03.056 [19] Kamiya H, Akhyari P, Martens A, et al. Sternal microcirculation after skeletonized versus pedicled harvesting of the internal thoracic artery: a randomized study[J]. J Thorac Cardiovasc Surg, 2008, 135(1): 32-7. doi: 10.1016/j.jtcvs.2007.09.004 [20] Benedetto U, Altman DG, Gerry S, et al. Pedicled and skeletonized single and bilateral internal thoracic artery grafts and the incidence of sternal wound complications: Insights from the arterial revascularization trial[J]. J Thorac Cardiovasc Surg, 2016, 152: 270-6. https://www.sciencedirect.com/science/article/pii/S0022522316300307 [21] Deutsch O, Gansera L, Wunderlich M, et al. Does bilateral ITA grafting increase perioperative complications? outcome of 6476 patients with bilateral versus 5020 patients with single ITA bypass [J]. Thorac Cardiovasc Surg, 2016, 64(3): 188-94. [22] Lepelletier D, Bourigault C, Roussel JC, et al. Epidemiology and prevention of surgical site infections after cardiac surgery[J]. Med Mal Infect, 2013, 43(10): 403-9. https://www.sciencedirect.com/science/article/pii/S0399077X13002011 [23] Gatti G, Maschietto L, Morosin M, et al. Routine use of bilateral internal thoracic artery grafting in women: a risk factor analysis for poor outcomes[J]. Cardiovasc Revasc Med, 2017, 18(1): 40-6. doi: 10.1016/j.carrev.2016.08.001 [24] Hashimoto M, Fukui T, Takanashi S. Bilateral internal thoracic artery grafting: is it reasonable in octogenarians[J]. Ann Thorac Cardiovasc Surg, 2015, 21(5): 452-8. doi: 10.5761/atcs.oa.14-00305 [25] 赵俊涛, 黄建岭, 张伟峰, 等.冠脉搭桥术后胸骨正中切口愈合不良相关因素分析[J].河南外科学杂志, 2017, 23(4): 29-30. http://d.old.wanfangdata.com.cn/Periodical/hnwkxzz201704016 [26] 邹小琴, 向海波.冠脉CTA及冠脉造影诊断冠心病价值比较[J].中国医疗设备, 2019, 34(S2): 132-3. https://kns.cnki.net/KCMS/detail/detail.aspx?dbcode=CJFD&filename=YLSX2019S2067 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 799
- HTML全文浏览量: 285
- PDF下载量: 4
- 被引次数: 0