



Application of multimodal ultrasound imaging technology in the diagnosis of diabetic peripheral neuropathy
-
摘要:
目的 探讨多模态超声成像技术在诊断糖尿病周围神经病变(DPN)中的应用。 方法 选取2019年1~10月我院2型糖尿病合并DPN患者38例(A组)、单纯2型糖尿病患者40例(B组)以及健康人群36例(C组),均给予常规二维超声、超声造影和剪切波超声弹性成像(SWE)等超声检查和神经电生理检查进行比较,利用受试者工作特征曲线(ROC)分析各参数对DPN诊断价值。 结果 A组胫神经运动神经动作电位潜伏期高于B、C组(P < 0.05),胚神经运动传导速度和波幅均低于B、C组(P < 0.05),B组和C组各项指标比较差异无统计学意义(P > 0.05);A组胫神经前后径、横径及横断面积均高于B、C组,且B组胫神经前后径、横径及横断面积高于C组,差异有统计学意义(P < 0.05);A组达峰时间高于B、C组,峰值强度和AUC低于B、C组,且B组达峰时间高于C组,峰值强度和AUC低于C组,差异有统计学意义(P < 0.05);A组胫神经弹性最大值(Emax)、最小值(Emin)和平均值(Emean)均高于B、C组,且B组胫神经Emax、Emin和Emean均高于C组,差异有统计学意义(P < 0.05);常规二维超声、超声造影和SWE扫描中分别以横断面积、峰值强度和Emean对DPN诊断效能最高,AUC分别为0.733、0.775和0.876,三者联合诊断AUC为0.948,灵敏度和特异度分别达83.78%和97.50%。 结论 多模态超声成像技术通过综合常规二维超声、超声造影和SWE等检查模式数据信息,可为评价DPN诊断提供周围神经形态特征、微循环血流灌注和弹性指标等参考依据。 Abstract:Objective To explore the application of multimodal ultrasound imaging technology (mUS) in the diagnosis of diabetic peripheral neuropathy (DPN). Methods From January 2019 to October 2019, 38 patients with T2DM and DPN (group A), 40 simple T2DM patients (group B) and 36 healthy people (group C) in our hospital were selected. They were given conventional two-dimensional ultrasound, ultrasound contrast and shear wave elastography (SWE) and neuroelectrophysiological examination. The results in different groups were compared. Receiver operating characteristic curve (ROC) was drawn and the area under the curve (AUC) was calculated to analyze the diagnostic value of each parameter on DPN. Results The incubation period in group A was significantly higher than that in groups B and C (P < 0.05). The MCV and amplitude were significantly lower than those in groups B and C (P < 0.05). The differences of the indicators between group B and group C were not significant(P > 0.05). The anterior-posterior diameter, transverse diameter and cross-sectional area of tibial nerve in group A were higher than those in groups B and C. The anterior-posterior diameter, transverse diameter and cross-sectional area of tibial nerve in group B were higher than those in group C (P < 0.05). Time to peak (TTP) in group A was higher than that in groups B and C, while the peak intensity (Imax) and AUC were lower than those in groups B and C. The TTP in group B was higher than that in group C, while the Imax and AUC were lower than those in group C(P < 0.05). The maximum (Emax), minimum (Emin) and mean value (Emean) of elasticity of tibial nerve in group A were higher than those in group B and C. The Emax, Emin and Emean of tibial nerve in group B were higher than those in group C (P < 0.05). The cross-sectional area, Imax and Emean had the highest diagnostic efficacy in diagnosing DPN in conventional two-dimensional ultrasound, ultrasound contrast and SWE, with AUC values of 0.733, 0.775 and 0.876. The AUC of combination of the three was 0.948. The sensitivity and specificity were up to 83.78% and 97.50%. Conclusions mUS technology can synthesize the data information of conventional two-dimensional ultrasound, ultrasound contrast and SWE examination models.It can provide reference basis for evaluating the diagnosis of DPN, such as peripheral nerve morphological characteristics, microcirculation blood perfusion and elasticity index. -

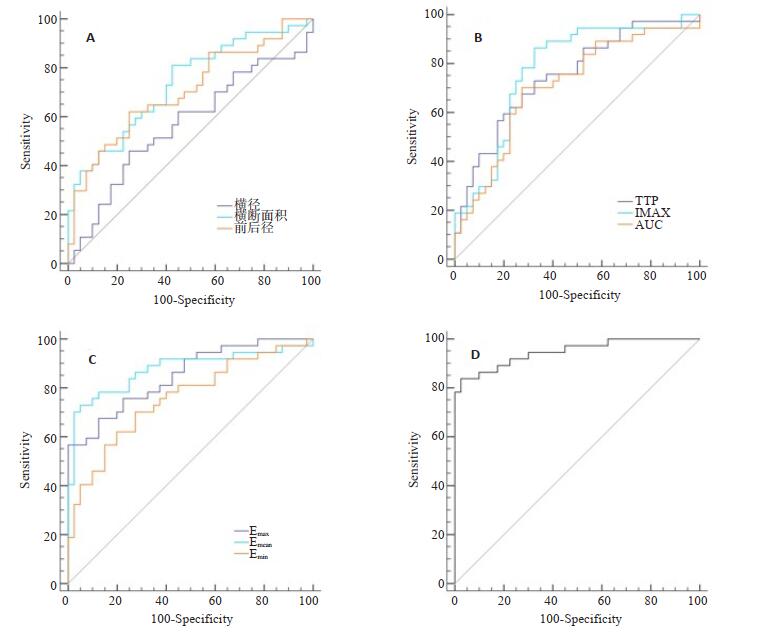
图 1 mUS对DPN鉴别诊断的ROC曲线
A:常规二维超声检测; B:超声造影; C: SWE扫描; D:横断面积、Imax和Emean联合诊断.
Figure 1. ROC curves of mUS in the differential diagnosis of DPN

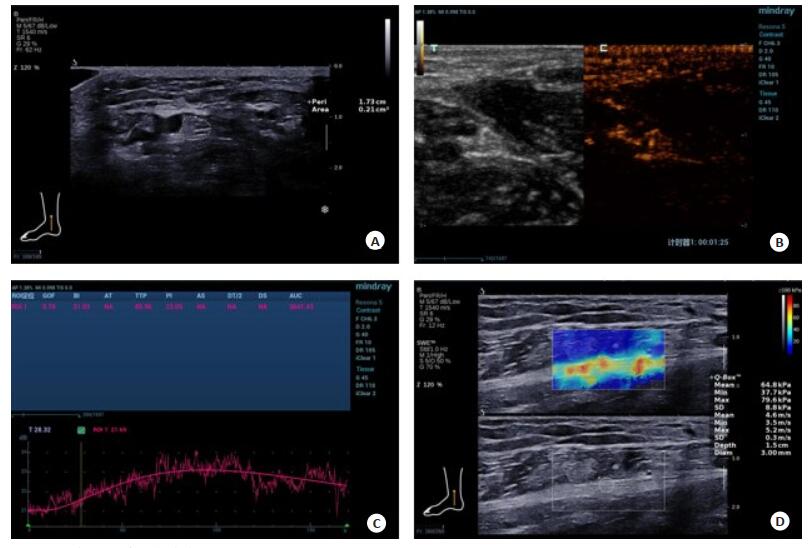
图 2 mUS在DPN检查中的应用
A:常规二维超声横切面扫描; B:超声造影检查; C:超声造影TIC曲线; D: SWE检查和胫神经弹性参数定量分析结果.
Figure 2. Application of mUS in DPN examination.
表 1 神经电生理指标比较
Table 1. Comparison of neuroelectrophysiological indexes (Mean±SD)
分组 潜伏期(ms) MCV (m/s) 波幅(mV) A组(n=38) 3.09±0.47 39.64±7.13 8.26±2.04 B组(n=40) 2.91±0.38* 47.82±6.25* 10.32±2.47* C组(n=36) 2.86±0.35* 49.01±4.98* 10.84±2.19* F 4.500 7.981 4.666 P 0.013 0.001 0.011 *P < 0.05 vs A组.MCV: Motor nerve conduction velocity.  下载: 导出CSV
下载: 导出CSV
表 2 常规二维超声测量结果比较
Table 2. Comparison of conventional two-dimensional ultrasound measurement results (Mean±SD)
分组 前后径(mm) 横径(mm) 横断面积(mm 2) A组(n=38) 3.89±0.41 6.25±0.78 21.06±4.18 B组(n=40) 3.56±0.32* 5.84±0.71* 16.72±3.59* C组(n=36) 3.07±0.28* # 5.36±0.60* # 15.91±2.85* # F 72.327 11.968 50.983 P 0.000 0.000 0.000 *P < 0.05 vs A组; #P < 0.05 vs B组.
下载: 导出CSV
表 3 超声造影测量结果比较
Table 3. Comparison of ultrasound contrast measurement results (Mean±SD)
分组 TTP (s) Imax (dB) AUC (dB·s) A组(n=38) 67.94±15.83 19.35±4.27 2835.06±712.49 B组(n=40) 56.12±13.26* 24.03±3.81* 3417.25±648.32* C组(n=36) 48.07±10.54* # 27.68±4.19* # 3902.84±654.17* # F 27.875 51.989 25.797 P 0.000 0.000 0.000 *P < 0.05 vs A组; #P < 0.05 vs B组.
下载: 导出CSV
表 4 SWE测量结果比较
Table 4. Comparison of SWE measurement results (Mean±SD, kPa)
分组 Emax Emin Emean A组(n=38) 51.83±14.25 32.06±9.12 43.29±8.74 B组(n=40) 36.79±10.36* 21.85±7.28* 30.67±6.38* C组(n=36) 27.48±8.92* # 17.43±6.05* # 24.81±6.45* # F 63.061 54.683 61.861 P 0.000 0.000 0.000 *P < 0.05 vs A组; #P < 0.05 vs B组.
下载: 导出CSV
表 5 常规二维超声、超声造影和SWE对DPN诊断价值分析
Table 5. Analysis of diagnostic value of conventional two-dimensional ultrasound, ultrasound contrast and SWE on DPN
参数 AUC SE 95%CI 最佳阈值 约登指数 灵敏度(%) 特异度(%) 常规二维超声 前后径 0.705 0.060 0.590~0.803 3.69 0.372 62.16 75.00 横径 0.567 0.067 0.449~0.679 6.32 0.209 45.95 75.00 横断面积 0.733 0.057 0.620~0.828 17.06 0.386 81.08 57.50 超声造影 TTP 0.749 0.056 0.637~0.841 60.90 0.405 72.97 67.50 Imax 0.775 0.055 0.666~0.862 22.16 0.539 86.49 67.50 AUC 0.709 0.060 0.594~0.807 3216.56 0.428 70.27 72.50 SWE Emax 0.851 0.043 0.751~0.922 49.43 0.568 56.76 100.00 Emin 0.727 0.056 0.646~0.848 28.29 0.428 70.27 72.50 Emean 0.876 0.044 0.782~0.940 40.29 0.679 72.97 95.00
下载: 导出CSV
-
[1] Gómez-Huelgas R, Gómez Peralta F, Rodríguez Maas L, et al. Treatment of type 2 diabetes mellitus in elderly patients[J]. Rev Esp Geriatr Gerontol, 2018, 53(2): 89-99. http://d.old.wanfangdata.com.cn/Periodical/zgjcyy201904004 [2] 中华医学会糖尿病学分会糖尿病教育与管理学组.中国2型糖尿病自我管理处方专家共识(2017年版[)J].中华糖尿病杂志, 2017, 9(12): 740-50. doi: 10.3760/cma.j.issn.1674-5809.2017.12.004 [3] Patel YR, Gadiraju TV, Gaziano JM, et al. Adherence to healthy lifestyle factors and risk of death in men with diabetes mellitus: The Physicians' Health Study[J]. Clin Nutr, 2018, 37(1): 139-43. doi: 10.1016/j.clnu.2016.11.003 [4] Feng YH, Chen L, Luo Q, et al. Involvement of microRNA-146a in diabetic peripheral neuropathy through the regulation of inflammation [J]. Drug Des Devel Ther, 2018, 12: 171-7. doi: 10.2147/DDDT.S157109 [5] Shabeeb D, Najafi M, Hasanzadeh G, et al. Electrophysiological measurements of diabetic peripheral neuropathy: a systematic review[J]. Diabetes Metab Syndr, 2018, 12(4): 591-600. https://www.researchgate.net/publication/324068687_Electrophysiological_measurements_of_diabetic_peripheral_neuropathy_A_systematic_review [6] 周静, 姜立新.超声评估糖尿病周围神经病变的研究进展[J].声学技术, 2019, 38(3): 307-11. http://d.old.wanfangdata.com.cn/Periodical/sxjs201903013 [7] Hong XW, Annamalai RT, Kemerer TS, et al. Multimode ultrasound viscoelastography for three-dimensional interrogation of microscale mechanical properties in heterogeneous biomaterials[J]. Biomaterials, 2018, 178: 11-22. doi: 10.1016/j.biomaterials.2018.05.057 [8] 中华医学会糖尿病学分会.中国2型糖尿病防治指南(2013年版[J].中国糖尿病杂志, 2014, 22(8): I0002-42. http://www.cnki.com.cn/Article/CJFDTotal-ZGTL201408030.htm [9] Vinik AI, Casellini CM. Guidelines in the management of diabetic nerve pain: clinical utility of pregabalin[J]. Diabetes Metab Syndr Obes, 2013, 6: 57-78. http://d.old.wanfangdata.com.cn/OAPaper/oai_doaj-articles_8ae043d5103d2cb34e18378759724334 [10] 马饶, 周显礼.糖尿病周围神经病变诊断方法的研究进展[J].医学综述, 2018, 24(17): 3462-6. doi: 10.3969/j.issn.1006-2084.2018.17.026 [11] 陈芮, 周显礼.超声在糖尿病周围神经病变诊断中的研究进展[J].临床超声医学杂志, 2019, 21(4): 288-90. doi: 10.3969/j.issn.1008-6978.2019.04.019 [12] Hong XW, Annamalai RT, Kemerer TS, et al. Multimode ultrasound viscoelastography for three-dimensional interrogation of microscale mechanical properties in heterogeneous biomaterials[J]. Biomaterials, 2018, 178: 11-22. doi: 10.1016/j.biomaterials.2018.05.057 [13] Huang YX, Hu B, Zhu JA. Study on the use of quantitative ultrasound evaluation of diabetic neuropathy in the rat sciatic nerve[J]. Australas Phys Eng Sci Med, 2016, 39(4): 997-1005. doi: 10.1007/s13246-016-0448-8 [14] Iqbal Z, Azmi S, Yadav R, et al. Diabetic peripheral neuropathy: epidemiology, diagnosis, and pharmacotherapy[J]. Clin Ther, 2018, 40(6): 828-49. doi: 10.1016/j.clinthera.2018.04.001 [15] 边红霞.糖尿病周围神经病的神经电生理特点分析[J].中国药物与临床, 2018, 18(3): 448-9. http://d.old.wanfangdata.com.cn/Periodical/jyjxxyxb201306016 [16] 孙冬梅, 王艳滨. 2型糖尿病伴周围神经病变胫神经的超声特征[J].中国医学影像学杂志, 2014(10): 781-3, 785. doi: 10.3969/j.issn.1005-5185.2014.10.016 [17] Arumugam T, Razali SN, Vethakkan SR, et al. Relationship between ultrasonographic nerve morphology and severity of diabetic sensorimotor polyneuropathy[J]. Eur J Neurol, 2016, 23(2): 354-60. doi: 10.1111/ene.12836 [18] Tu YJ, Chen ZG, Hu JD, et al. Chronic nerve compression accelerates the progression of diabetic peripheral neuropathy in a rat model: a study of gene expression profiling[J]. J Reconstr Microsurg, 2018, 34(7): 537-48. doi: 10.1055/s-0038-1642023 [19] Qureshi AI, Saleem MA, Ahrar A, et al. Imaging of the Vasa nervorum using contrast-enhanced ultrasound[J]. J Neuroimaging, 2017, 27(6): 583-8. doi: 10.1111/jon.12429 [20] Jiang WX, Huang SR, Teng H, et al. Diagnostic performance of two-dimensional shear wave elastography for evaluating tibial nerve stiffness in patients with diabetic peripheral neuropathy[J]. Eur Radiol, 2019, 29(5): 2167-74. doi: 10.1007/s00330-018-5858-4 [21] Petropoulos IN, Tavakoli M, Marshall A, et al. Response to comment on Malik. Which test for diagnosing early human diabetic neuropathy[J]. Diabetes, 2015, 64(2): e2-8. doi: 10.2337/db14-1608 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 595
- HTML全文浏览量: 362
- PDF下载量: 9
- 被引次数: 0