



Clinical effect of double endobutton plate and clavicular hook platefixation on treatment of Tossy Ⅲ type acromioclavicular joint dislocation
-
摘要:
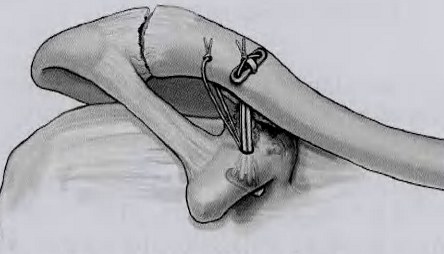
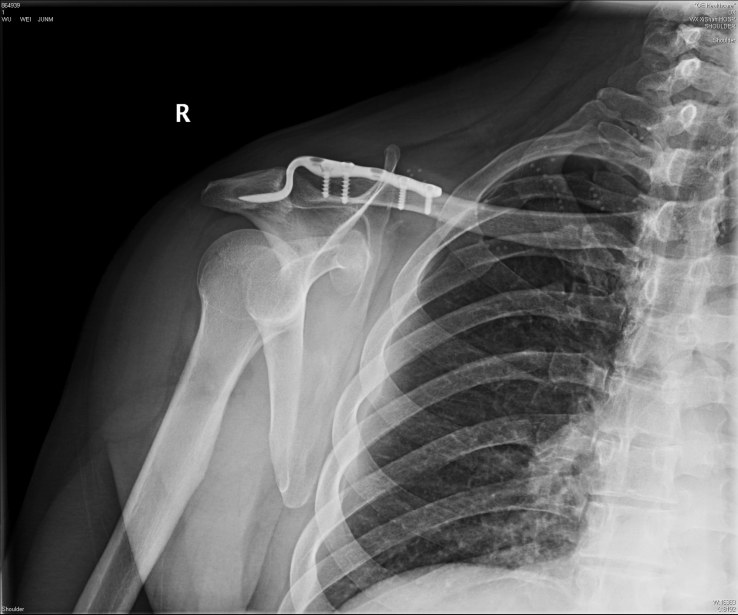
目的探讨双Endobutton纽扣钢板和锁骨钩钢板治疗TossyⅢ型肩锁关节脱位的临床疗效。 方法回顾分析2011年6月~2016年6月无锡市锡山人民医院收治的40例TossyⅢ型肩锁关节脱位患者,其中男性22例,女性18例,年龄21~57岁,平均33岁,伤后至手术时间1~4 d,平均2 d,术后抗生素使用不超过3 d。根据手术方式的不同分为两组:双Endobutton纽扣钢板组20例,锁骨钩钢板组20例,分别观察手术切口、手术时间、术中出血量、术后并发症发生率、术后肩关节功能恢复情况等。 结果Endobutton纽扣钢板组在手术切口,手术时间,术中出血量,术后并发症发生率,术后肩关节功能恢复情况方面,与锁骨钩钢板组比较有统计学差异(P < 0.05),所有患者切口均Ⅰ期愈合,无血管神经损伤及感染等早期并发症,每位患者均获随访,随访时间为3~24个月。随访期间所有患者无内固定松动及脱出,无关节再脱位发生。 结论双Endobutton技术是治疗TossyⅢ型肩锁关节脱位的一种非常有效的 方法,它手术切口小,操作简单,临床效果满意,适合基层医院推广。 -
关键词:
- 肩锁关节脱位 /
- 双Endobutton纽扣钢板 /
- 锁骨钩钢板
Abstract:ObjectiveTo explore the clinical efficacy of the double Endobutton plate and Clavicular Hook Plate fixation treatment for Tossy Ⅲ acromioclavicular joint dislocation. MethodsFrom June 2011 to June 2016, 40 patients of Tossy Ⅲ acromioclavicular joint dislocation admitted to the wuxi xishan hospital were enrolled, including 12 males and 8 females, aged from 21 to 55 years old with an average age of 33.The time from injury to operation was 1-4 days, averaged 2 days, the application of antibiotics was no more than 3 days after operation. They were divided into two groups according to the different methods of operation: double endobutton plate group with 20 cases and clavicular hook plate group with 20 cases. ResultsCompared with clavicular hook plate group, double endobutton plate group had significant difference in incision, operation time, intraoperative blood loss, shoulder 's function recovery (P < 0.05).All patients'incisions were healed well, with no early complications such as blood vessels and nerves'injury and postoperative infection. The patients were followed up from 3 to 24 months, there was no internal fixation loosening and joint dislocation were occured during the follow-up period. ResultsDouble Endobutton technique is an effective method on treatment of Tossy Ⅲ type acromioclavicular joint dislocation with minimal invasive, simple operation and satisfied clinical effect.It is suitable for basic-level hospital. -
表 1 2组患者基本情况的比较(n=20)
组别 年龄(岁) 体质量(kg) 性别比例(女/男) Endobutton组 32.4±9.14 59.1±6.01 8/12 锁骨钩钢板组 33.65±9.48 60.4±6.25 9/11 t/χ2 -0.424 -0.67 0.102 P 0.674 0.507 0.749  下载: 导出CSV
下载: 导出CSV
表 2 2组在术中术后情况的比较
组别 切口长度(cm) 手术时间(min) 术中出血量(mL) Endobutton组 4.65±0.67* 68.75±10.87* 15.75±6.34* 锁骨钩钢板组 7.35±0.49 48±12.18 39.75±7.86 t -14.54 5.684 -10.629 P 0.000 0.000 0.000 *P<0.01 vs 锁骨钩钢板组.
下载: 导出CSV
表 3 2组患者在肩关节功能方面的比较(n,%)
组别 痊愈 有效 无效 有效率 Endobutton组 15(75) 4(20) 1(5) 19(95*) 锁骨钩钢板组 5(25) 8(40) 7(35) 13(65) χ2 5.625 P 0.018 *P<0.05 vs 锁骨钩钢板组.
下载: 导出CSV
-
[1] Alyas F, Curtis M, Speed C, et al. Mr imaging appearances of acromioclavicular joint dislocation[J]. Radiographics, 2008, 28(2):463-79. doi: 10.1148/rg.282075714 [2] Kim AC, Matcuk G, Patel D, et al. Acromioclavicular joint injuries and reconstructions: a review of expected imaging findings and potential complications[J]. Emerg Radiol, 2012, 19(5): 399-413. doi: 10.1007/s10140-012-1053-0 [3] Struhl S. Double endobutton technique for repair of complete acromioclavicular joint dislocations[J]. Tech Shoulder Elbow Surg,2007, 8(4): 175-9. doi: 10.1097/BTE.0b013e31815907a3 [4] 汪李军, 杨惠林, 史源欣, 等. 双Endobutton 技术与锁骨钩钢板治疗Tossy Ⅲ型肩锁关节脱位的疗效比较[J]. 中华创伤骨科杂志, 2013,15(4): 283-7. http://cn.bing.com/academic/search?q=%e4%b8%ad%e5%8d%8e%e5%88%9b%e4%bc%a4%e9%aa%a8%e7%a7%91%e6%9d%82%e5%bf%97&FORM=AJOUR [5] 郭丹, 周海斌. Rockwood Ⅲ型肩锁关节脱位两种治疗方法分析[J].安徽医药, 2013, 17(3): 460-1. http://www.cnki.com.cn/Article/CJFDTOTAL-AHYY201303045.htm [6] Ejam S, Lind T, Falkenberg B. Surgical treatment of acute and chronic acromioclavicular dislocation Tossy type Ⅲ and V using the Hook plate[J]. Acta Orthop Belg, 2008, 74(4): 441-5. [7] 曾纪洲, 曲铁兵, 潘江, 等. 锁骨钩钢板固定治疗Ⅲ度肩锁关节脱位[J]. 中华创伤杂志, 2002, 18(9): 547-50. http://www.cnki.com.cn/Article/CJFDTOTAL-ZHCS200209011.htm [8] Nuechtern JV, Sellenschloh K, Bishop N, et al. Biomechanical evaluation of 3 stabilization methods on acromioclavicular joint dislocations[J]. Am J Sports Med, 2013, 41(6): 1387-94. doi: 10.1177/0363546513484892 [9] Nadarajah R, Mahaluxmivala J, Amin A, et al. Clavicular hook-plate: complications of retaining the implant[J]. Injury, 2005,36(5): 681-3. doi: 10.1016/j.injury.2004.08.010 [10] Chaudry SN, Waseem M. Clavicular hook plate:complications of retaining the implant [J]. Injury, 2006, 37(7): 665-8. http://cn.bing.com/academic/profile?id=c6a52503d7fe8bd4e61426b95ac4dbaa&encoded=0&v=paper_preview&mkt=zh-cn [11] Tossy JD, Mead NC, Sigmond HM. Acromioclavicular separations,usefull and practical ciassification for treatment[J]. Clin Orthop,1963, 28(6): 111-9. http://cn.bing.com/academic/profile?id=fc69acafd4a497ff75fa3a17c844e36c&encoded=0&v=paper_preview&mkt=zh-cn [12] 胡晓波, 蒋电明, 阳明明, 等. 双带袢纽扣钢板与锁骨钩钢板治疗TossyⅢ型肩锁关节脱位的疗效评价[J]. 中华创伤杂志, 2014, 30(10): 1009-13. [13] Ye G, Peng C, Sun HB, et al. Treatment of rockwood type III acromioclavicular joint dislocation usingautogenoussemitendinos us tendon graft and endobutton techniqu[J]. Clin Risk Manag,2016, 12(3): 47-51. [14] Grantham C, Heckmann N, Wang L, et al. A biomechanical assessment of a novel double endobutton technique versus a coracoid cerclage sling for acromioclavicular and coracoclavicular injuries[J]. Knee Surg Sports Traumatol Arthrosc, 2016, 24(6):1918-24. doi: 10.1007/s00167-014-3198-8 [15] Struhl S, Wolfson TS. Continuous loop double endobutton reconstruction for acromioclavicular joint dislocation[J]. Am J Sports Med, 2015, 43(10): 2437-40. doi: 10.1177/0363546515596409 -




 点击查看大图
点击查看大图

图(6) / 表(3)
计量
- 文章访问数: 595
- HTML全文浏览量: 309
- PDF下载量: 0
- 被引次数: 0