



The value of transthoracic echocardiography in the diagnosis of type A aortic dissection: a Meta analysis of prospective study
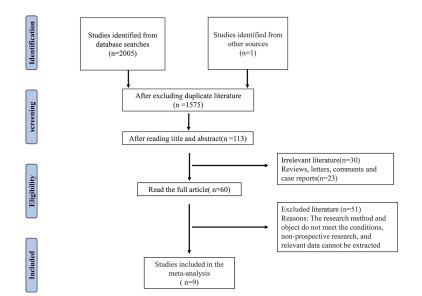
-
摘要:
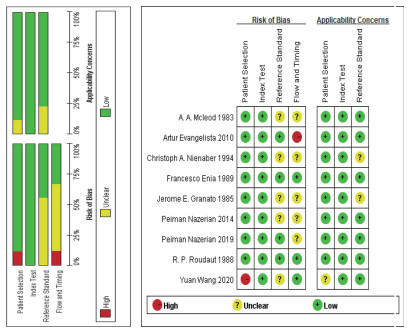
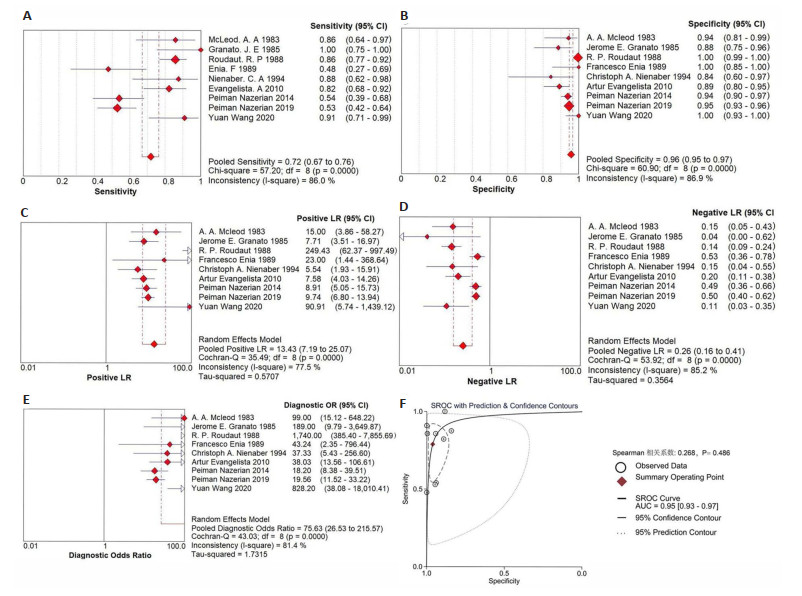
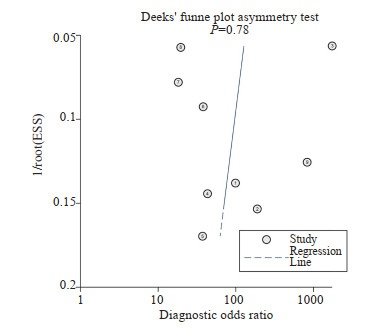
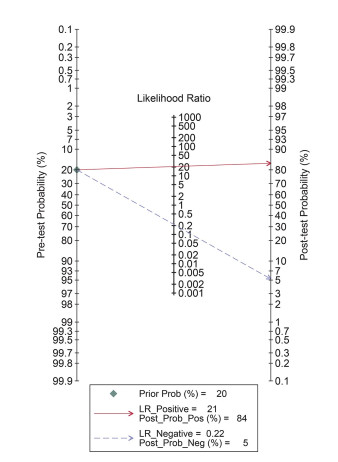
目的 通过Meta分析方法评估经胸超声心动图对Stanford A型主动脉夹层(AAD)的诊断效能。 方法 运用Meta-disc1.4和Stata16.0对纳入文献的9组数据的真阳性数、假阳性数、真阴性数、假阴性数进行分析,对敏感度、特异性、阳性似然比、阴性似然比、诊断比值比的合并效应值进行估计,通过汇总ROC曲线下面积和Fagan列线图估计经胸超声心动图的诊断准确度。采用单因素Meta回归探索异质性来源,通过Deeks'漏斗图不对称试验检验发表偏倚。 结果 敏感度的合并效应值为0.72(95% CI: 0.67~0.76),特异性的合并效应值为0.96(95% CI: 0.95~0.97),阳性似然比为13.43(95% CI: 7.19~25.07),阴性似然比为0.26(95% CI: 0.16~0.41),诊断比值比高达75.63(95% CI: 26.53~215.57),汇总ROC曲线下面积为0.95 (95% CI: 0.93~0.97),Fagan图中验后概率由验前的20%提升至84%。敏感度和特异性Q检验结果显示存在异质性(P < 0.01)。Meta回归显示样本量、人群年龄、超声技术、操作人群、超声诊断标准选择、金标准选择并非是异质性来源;进一步分析显示超声阳性标准设置严格和操作人群缺乏经验均使诊断敏感度过低,可能是本文的异质性来源。Deeks'漏斗图显示纳入的9篇文献不存在发表偏倚(P=0.78)。 结论 经胸超声心动图对AAD具有较高的诊断效能,可作为AAD的初步影像学评估手段。亚组分析提示通过调整超声阳性标准设定以及加强操作人员相关培训可能会减少对AAD的漏诊,进一步提高诊断敏感度。 Abstract:Objective Meta-analysis was used to systematically review the diagnostic efficacy of transthoracic echocardiography on type A aortic dissection (AAD). Methods The Meta-disc1.4 and Stata 16.0 software was used to analyze 9 literatures as well as 9 groups of data including true positive, false positive, true negative and false negative values, and estimated the combined effect values of sensitivity, specificity, positive likelihood ratio, negative likelihood ratio and diagnostic odds ratio were estimated. The area under curve of the summary ROC curve and the Fagan nomogram were summarized to estimate the diagnostic accuracy of transthoracic echocardiography. The sources of heterogeneity were analyzed by Meta-regression analysis. Deeks' funnel diagram asymmetry test was used to test publication bias. Results The combined value of sensitivity was 0.72 (95%CI: 0.67-0.76), specificity was 0.96 (95% CI: 0.95-0.97), positive likelihood ratio was 13.43 (95%CI: 7.19-25.07), negative likelihood ratio was 0.26 (95%CI: 0.16-0.41)and the area under curve was 0.95 (95%CI: 0.93-0.97). The post-test probability increased from 20% to 84% in Fagan nomogram, all indicating a high diagnostic accuracy. Sensitivity and specificity Q test were less than 0.01, which indicated some heterogeneity. Meta-regression showed that sample size, age of population, ultrasound technology, operator population, selection of ultrasound diagnostic criteria and selection of gold standard were not the sources of heterogeneity. However, Subgroup analysis showed that the strict setting of ultrasound positive criteria and the lack of experience in the operator population made the diagnostic sensitivity too low, which may be the source of heterogeneity in our study. Deeks' funnel plot showed that there was no publication bias for the 9 included literatures (P=0.78). Conclusion Transthoracic echocardiography has high diagnostic efficacy for AAD and can be used as a preliminary imaging evaluation method for AAD. However, it may be necessary to adjust the setting of ultrasound positive criteria and strengthen the relevant training of operators to reduce the missed diagnosis of AAD and further improve the diagnostic sensitivity. -

图 4 敏感度(A)、特异性(B)、阳性似然比(C)、阴性似然比(D),诊断比值比(E)合并效应的森林图及汇总ROC曲线(F)
Figure 4. Forest plots of Sensitivity (A), Specificity (B), PLR (C), NLR (D), DOR (E) and SROC curve (F).
表 1 纳入文献基本特征
Table 1. Basic characteristics of the included literature
Author Year Type Country n Average age (year) True positive(n) False positive(n) False negative(n) True negative(n) Operator Doppler Positive criteria * Gold standard ** A. A. Mcleod[16] 1983 Prospective USA 56 58.7 18 2 3 33 1 No 2 2 Jerome E. Granato[17] 1985 Prospective USA 56 60.8 13 5 0 38 1 No 2 2 R. P. Roudaut[18] 1988 Prospective France 673 62 78 2 13 580 2 No 2 2 Francesco Enia[19] 1989 Prospective Italy 46 57.9 11 0 12 23 1 No 3 1 Christoph A. Nienaber[20] 1994 Prospective Germany 35 51 14 3 2 16 1 Yes 2 2 Artur Evangelista[21] 2010 Prospective Spain 128 61 37 9 8 74 1 Yes 1 2 Peiman Nazerian[22] 2014 Prospective Italy 281 67.7 27 14 23 217 2 Yes 2 2 Peiman Nazerian[23] 2019 Prospective Italy 839 62 45 41 40 713 2 Yes 2 2 Yuan Wang[24] 2020 Prospective China 72 52.7 20 0 2 50 2 Yes 1 1 *Ultrasonic positive standard:1=The aortic intimal separation is floating and oscillating in bands or lines of echo;2=The aortic intimal separation is floating and oscillating in bands or lines of echo+ any of the following:Widening diameter of ascending aorta root >42 mm, pericardial effusion/signs of cardiac tamponade, color Doppler indicates aortic regurgitation;3=The aortic intimal separation is floating and oscillating in bands or lines of echo + widening of ascending aorta root, diameter>42 mm + hydropericardium/signs of cardiac tamponade; **Diagnostic gold standard: 1=Diagnosis by imaging only; 2=Diagnosis by multiple methods (image, operation, autopsy, etc).  下载: 导出CSV
下载: 导出CSV
表 2 Meta回归分析
Table 2. Meta-regression analysis
Inclusion factor Relative diagnostic odds ratio (95% CI) P Age 0.95 (0.63-1.43) 0.745 Sample size 1.00 (0.99-1.01) 0.881 Operator 1.34(0.02-94.49) 0.871 Ultrasonic equipment 0.13(0.01-1.27) 0.071 Ultrasonic diagnostic criteria 0.48(0.02-10.49) 0.578 Gold standard 0.47(0.00-44.30) 0.696 literature(3 vs 6) 0.05(0.01-0.20) 0.002
下载: 导出CSV
表 3 敏感度分析
Table 3. Sensitivity analysis
Literature exclusion Sensitivity(95% CI) Specificity(95% CI) A. A. Mcleod 1983 71%(66%-76%) 96%(95%-97%) Jerome E. Granato 1985 71%(66%-76%) 96%(95%-97%) R. P. Roudaut 1988 67%(61%-73%) 94%(93%-95%) Francesco Enia 1989 73%(68%-78%) 96%(95%-97%) Christoph A. Nienaber 1994 71%(66%-76%) 96%(95%-97%) Artur Evangelista 2010 70%(65%-75%) 96%(95%-97%) Peiman Nazerian 2014 75%(70%-79%) 96%(95%-97%) Peiman Nazerian 2019 78%(72%-82%) 97%(95%-98%) Yuan Wang 2020 71%(66%-75%) 96%(95%-97%)
下载: 导出CSV
-
[1] Hagan PG, Nienaber CA, Isselbacher EM, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease[J]. JAMA, 2000, 283(7): 897-903. doi: 10.1001/jama.283.7.897 [2] Pape LA, Awais M, Woznicki EM, et al. Presentation, diagnosis, and outcomes of acute aortic dissection[J]. J Am Coll Cardiol, 2015, 66(4): 350-8. doi: 10.1016/j.jacc.2015.05.029 [3] Eranki A, Merakis M, Williams ML, et al. Outcomes of surgery for acute type A dissection in octogenarians versus non-octogenarians: a systematic review and meta analysis[J]. J Cardiothorac Surg, 2022, 17(1): 222. doi: 10.1186/s13019-022-01980-x [4] Duan WX, Wang WG, Xia L, et al. Clinical profiles and outcomes of acute type A aortic dissection and intramural hematoma in the current era: lessons from the first registry of aortic dissection in China[J]. Chin Med J, 2021, 134(8): 927-34. doi: 10.1097/CM9.0000000000001459 [5] Li QG, Yu WD, Ma WG. Large clinical registries for acute aortic dissection: interpretation and comparison of latest results[J]. Zhonghua Wai Ke Za Zhi, 2019, 57(5): 326-30. [6] Nienaber CA, Clough RE. Management of acute aortic dissection[J]. Lancet, 2015, 385(9970): 800-11. doi: 10.1016/S0140-6736(14)61005-9 [7] Huang LT, Tsai YS, Liou CF, et al. Automated Stanford classification of aortic dissection using a 2-step hierarchical neural network at computed tomography angiography[J]. Eur Radiol, 2022, 32(4): 2277-85. doi: 10.1007/s00330-021-08370-2 [8] Mussa FF, Horton JD, Moridzadeh R, et al. Acute aortic dissection and intramural hematoma: a systematic review[J]. JAMA, 2016, 316(7): 754-63. doi: 10.1001/jama.2016.10026 [9] Parve S, Ziganshin BA, Elefteriades JA. Overview of the current knowledge on etiology, natural history and treatment of aortic dissection[J]. J Cardiovasc Surg, 2017, 58(2): 238-51. [10] Minatoya K. The reality of the treatment for acute aortic dissection in a megacity[J]. Eur J Cardiothorac Surg, 2021, 60(4): 965-6. doi: 10.1093/ejcts/ezab261 [11] Ahlsson A, Wickbom A, Geirsson A, et al. Is there a weekend effect in surgery for type A dissection?: results from the Nordic consortium for acute type A aortic dissection database[J]. Ann Thorac Surg, 2019, 108(3): 770-6. doi: 10.1016/j.athoracsur.2019.03.005 [12] Su IM, Huang HK, Liu PPS, et al. Mortality risk from acute aortic dissection among hospital admissions during weekends and holiday season[J]. PLoS One, 2021, 16(9): e0255942. doi: 10.1371/journal.pone.0255942 [13] Krapf L, Vahanian A, Messika-Zeitoun D. Three-dimensional transoesophageal echocardiography in aortic dissection[J]. Heart, 2009, 95(1): 55. doi: 10.3969/j.issn.1009-0126.2009.01.019 [14] Flachskampf FA, Wouters PF, Edvardsen T, et al. Recommendations for transoesophageal echocardiography: EACVI update 2014[J]. Eur Heart J Cardiovasc Imaging, 2014, 15(4): 353-65. doi: 10.1093/ehjci/jeu015 [15] Diaz A, Martin-Raymondi D, Barba J. Complete aortic dissection demonstrated by intraoperative transoesophageal echocardiography[J]. Heart, 2005, 91(1): 101. doi: 10.1136/hrt.2004.036194 [16] McLeod AA, Monaghan MJ, Richardson PJ, et al. Diagnosis of acute aortic dissection by M-mode and cross-sectional echocardiography: a five-year experience[J]. Eur Heart J, 1983, 4(3): 196-202. doi: 10.1093/oxfordjournals.eurheartj.a061439 [17] Granato JE, Dee P, Gibson RS. Utility of two-dimensional echocardiography in suspected ascending aortic dissection[J]. Am J Cardiol, 1985, 56(1): 123-9. doi: 10.1016/0002-9149(85)90579-X [18] Roudaut RP, Billes MA, Gosse P, et al. Accuracy of m-mode and two-imensional echocardiography in the diagnosis of aortic dissection: an experience with 128 cases[J]. Clin Cardiol, 1988, 11(8): 553-62. doi: 10.1002/clc.4960110809 [19] Enia F, Ledda G, Mauro RL, et al. Utility of echocardiography in the diagnosis of aortic dissection involving the ascending aorta[J]. Chest, 1989, 95(1): 124-9. doi: 10.1378/chest.95.1.124 [20] Nienaber CA, von Kodolitsch Y, Brockhoff CJ, et al. Comparison of conventional and transesophageal echocardiography with magnetic resonance imaging for anatomical mapping of thoracic aortic dissection[J]. Int J Cardiac Imag, 1994, 10(1): 1-14. doi: 10.1007/BF01151576 [21] Evangelista A, Avegliano G, Aguilar R, et al. Impact of contrast-enhanced echocardiography on the diagnostic algorithm of acute aortic dissection[J]. Eur Heart J, 2009, 31(4): 472-9. [22] Nazerian P, Vanni S, Castelli M, et al. Diagnostic performance of emergency transthoracic focus cardiac ultrasound in suspected acute type A aortic dissection[J]. Intern Emerg Med, 2014, 9(6): 665-70. doi: 10.1007/s11739-014-1080-9 [23] Nazerian P, Mueller C, Vanni S, et al. Integration of transthoracic focused cardiac ultrasound in the diagnostic algorithm for suspected acute aortic syndromes[J]. Eur Heart J, 2019, 40(24): 1952-60. doi: 10.1093/eurheartj/ehz207 [24] Wang Y, Yu H, Cao Y, et al. Early screening for aortic dissection with point-of-care ultrasound by emergency physicians: a prospective pilot study[J]. J Ultrasound Med, 2020, 39(7): 1309-15. doi: 10.1002/jum.15223 [25] 练睿, 闫圣涛, 张素巧, 等. 经胸心脏超声对A型急性主动脉夹层诊断价值的荟萃分析[J]. 中华急诊医学杂志, 2016, 25(10): 1284-90. doi: 10.3760/cma.j.issn.1671-0282.2016.10.014 [26] Whiting PF, Rutjes AWS, Westwood ME, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies[J]. Ann Intern Med, 2011, 155(8): 529-36. doi: 10.7326/0003-4819-155-8-201110180-00009 [27] Aboyans V, Boukhris M. Dissecting the epidemiology of aortic dissection[J]. Eur Heart J Acute Cardiovasc Care, 2021, 10(7): 710-1. doi: 10.1093/ehjacc/zuab065 [28] Nakai C, Izumi S, Haraguchi T, et al. Acute type A aortic dissection with cardiopulmonary arrest at presentation[J]. Ann Thorac Surg, 2021, 112(4): 1210-6. doi: 10.1016/j.athoracsur.2020.11.007 [29] Cuellar-Calabria H, Burcet G, Roque A, et al. Differences in the area of proximal and distal entry tears at CT angiography predict long-term clinical outcomes in aortic dissection[J]. Radiol Cardiothorac Imaging, 2021, 3(6): e210029. doi: 10.1148/ryct.2021210029 [30] Yao ZY, Xie W, Zhang JW, et al. ImageTBAD: a 3D computed tomography angiography image dataset for automatic segmentation of type-B aortic dissection[J]. Front Physiol, 2021, 12: 732711. doi: 10.3389/fphys.2021.732711 [31] Nienaber CA. The role of imaging in acute aortic syndromes[J]. Eur Heart J Cardiovasc Imaging, 2012, 14(1): 15-23. [32] Litmanovich D, Bankier AA, Cantin L, et al. CT and MRI in diseases of the aorta[J]. AJR Am J Roentgenol, 2009, 193(4): 928-40. doi: 10.2214/AJR.08.2166 [33] Huang F, Wu H, Lai QQ, et al. Application value of preoperative dual-source computed tomography in assessing the rupture site of thoracic aortic dissection[J]. J Cardiothorac Surg, 2021, 16(1): 346. doi: 10.1186/s13019-021-01729-y [34] 中国医师协会心血管外科分会大血管外科专业委员会, 张宏家, 孙立忠, 等. 急性主动脉综合征诊断与治疗规范中国专家共识(2021版)[J]. 中华胸心血管外科杂志, 2021, 37(5): 257-69. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 107
- HTML全文浏览量: 76
- PDF下载量: 8
- 被引次数: 0