



Value of novel stereotactic puncture technique in puncture drainage of hypertensive intracerebral hemorrhage patients
-
摘要:
目的 评价新型立体定向穿刺技术在高血压脑出血穿刺引流中的应用价值。 方法 选取我院自2017年1月~2021年1月收治的24例使用该技术进行血肿穿刺引流的脑出血患者的临床资料进行回顾性分析,观察其穿刺的精准度、血肿清除率、手术前后格拉斯哥昏迷评分以及并发症的发生情况,进一步探讨该技术的临床应用价值。 结果 24例患者术后复查头颅CT均可见引流管放置位置良好,均沿着血肿长轴放置且尖端位于血肿内,与术前拟定血肿穿刺靶点位置的偏移距离为4.53±3.40 mm,均≤10 mm,术后血肿清除满意,无患者术后出现再出血及导管相关性感染。 结论 该立体定向穿刺技术操作简单、定位准确,可以节省手术及术前准备时间,保证血肿穿刺的成功率及准确性,且手术创伤及术后并发症较少,再出血风险低,适用于脑出血急症。 Abstract:Objective To evaluate the application value of the novel stereotactic puncture technique in hypertensive intracerebral hemorrhage drainage. Methods Clinical data of 24 patients who underwent hematoma puncture and drainage using this technique at our hospital from January 2017 to January 2021 were retrospectively analyzed. The puncture accuracy, hematoma clearance rate, pre- and postoperative Glasgow coma scale score, and the incidence of complications were observed to further investigate the clinical value of this technique. Results In all 24 cases, postoperative cranial CT scans showed good placement of the drainage tube, all along the long axis of the hematoma with the tip inside the hematoma. The offset distance from the preoperative target point was 4.53±3.40 mm, all≤10 mm. The hematoma clearance was satisfactory postoperatively and there were no instances of re-bleeding or catheter-related infections. Conclusion This stereotactic puncture technique is simple to operate and accurately positioned, which can save surgery and preoperative preparation time, ensure the success rate and accuracy of hematoma puncture, and reduce surgical trauma and postoperative complications, with a low risk of re-bleeding. It is suitable for emergency cases of cerebral hemorrhage. -

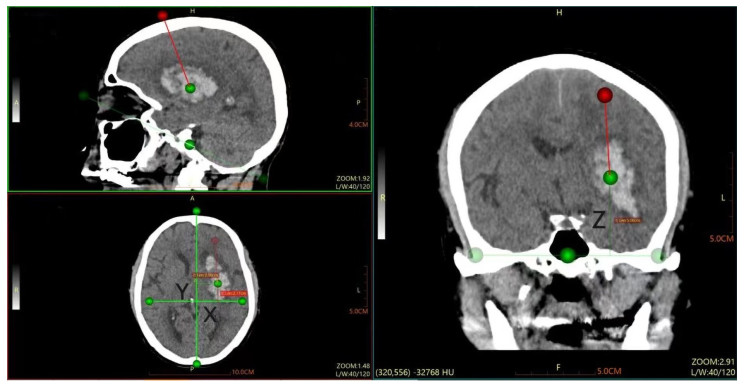
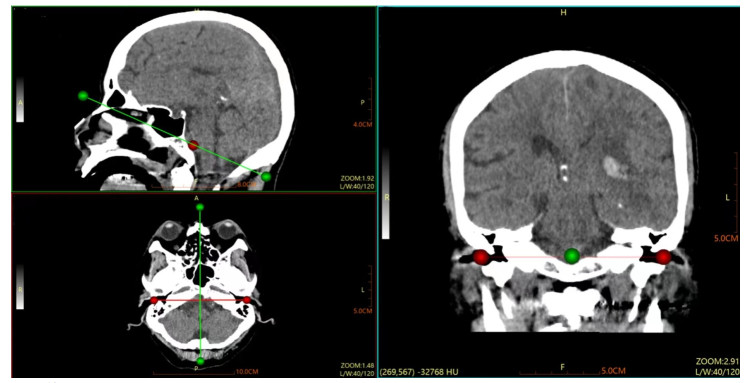
图 2 靶点层面显示靶点坐标(X1,Y1,Z1)及穿刺方向
Figure 2. Target plane shows the target coordinates(X1, Y1, Z1)and the puncture direction.

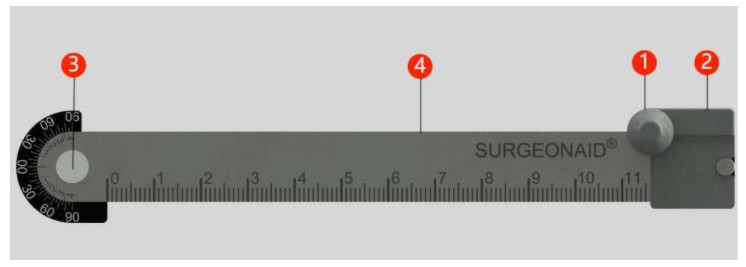
图 3 定位尺重叠位置
Figure 3. Overlap position of positioning ruler. ①Earplug; ②The slider can be moved; ③Axis of rotation with measurement angle; ④Two rulers overlapping.

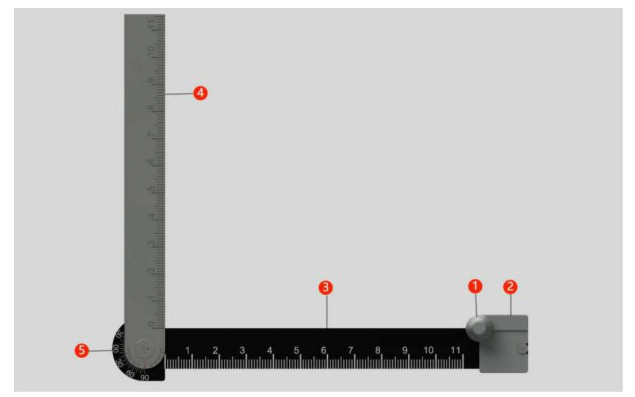
图 4 定位尺展开位置
Figure 4. Unfolded position of positioning ruler. ①Earplug; ②The slider can be moved; ③Ruler 1;④Ruler 2; ⑤Axis of rotation with measurement angle.

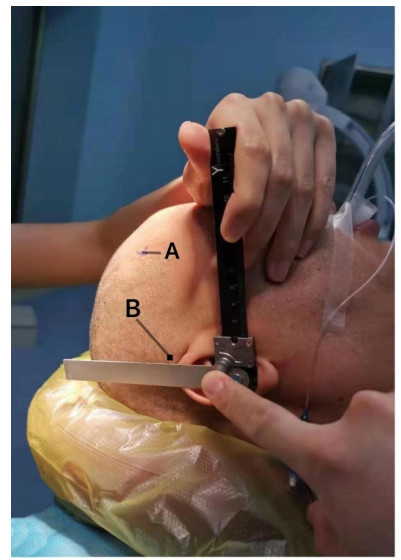
图 5 显示定位尺的操作
Figure 5. Displays the operation of the positioning ruler. A: Puncture point; B: Projection of the target in the temporal region. The picture showed two rulers perpendicular to each other, the direction of the black ruler was the direction of the OML, and the scale Z1 on the silver ruler was the position of the target on the body surface of one temporal region. For hematomas located in the basal ganglia and thalamus, we generally used the area in front of the coronal suture behind the hairline as the site of skull drilling.

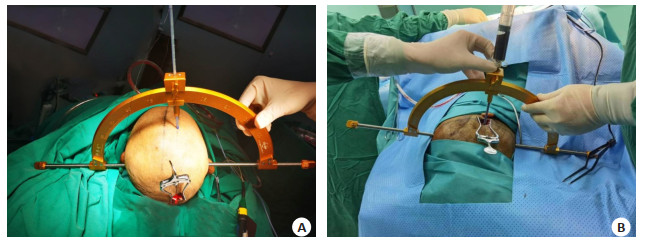
图 6 颅脑穿刺导引器的安装与使用
Figure 6. Installation and use of cranial puncture guide. A: Drawing a median sagittal line on the scalp and a parallel line parallel to the median sagittal line on the hematoma side, with a distance of X from the median sagittal line, and pointing the cranial puncture guide at an angle of 0°to this line; B: The precise positioning of surgery and the process of intraoperative hematoma aspiration.

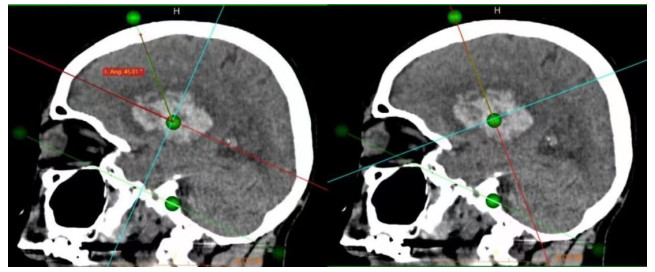
图 7 矢状面,穿刺方向与听眦线夹角为45.01°,旋转十字游标至S层面
Figure 7. Sagittal plane, the angle between the puncture direction and the canthal line is 45.01°, and the cross cursor was rotated to the S plane.

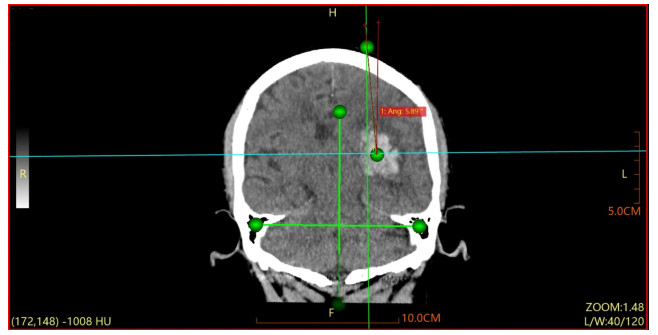
图 8 以S平面为扫描基线得到的穿刺平面,穿刺方向与正中矢状线的夹角,即5.89°
Figure 8. The angle between the puncture direction and the median sagittal line obtained by taking the S plane as the scanning baseline, that was, 5.89°.

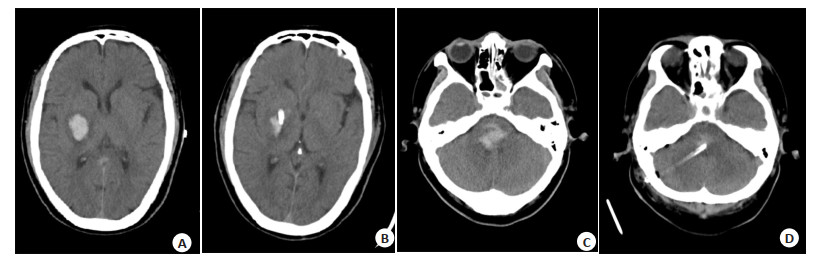
图 9 颅内血肿清除示意图
Figure 9. Illustration of intracranial hematoma removal. A, C: Preoperative CT; B, D: Repeat CT on the first day after surgery.

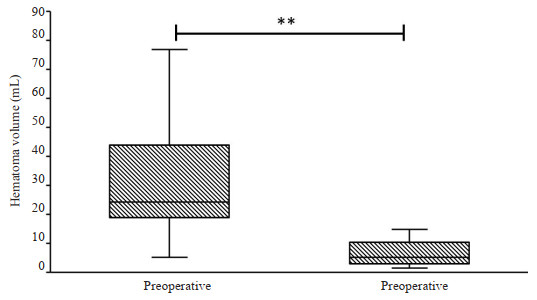
图 10 手术前后血肿量比较
Figure 10. Comparison of hematoma volume before and after surgery. The average volume of preoperative hematoma was 29.35±17.77 mL, the average volume of residual hematoma was 8.81±8.75 mL after the first postoperative CT examination, and the average volume of postoperative hematoma removal was 20.54±2.93 mL. There were statistical differences in the amount of hematoma before and after surgery. Z=-4.286, **P < 0.01.

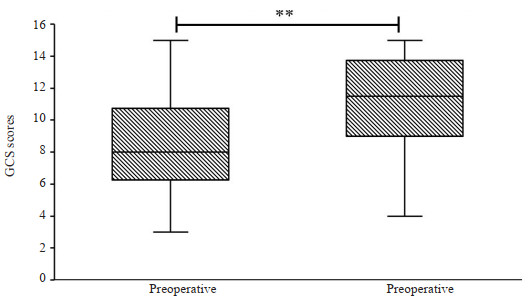
图 11 手术前后GCS评分比较
Figure 11. Comparison of GCS scores before and after surgery. The average preoperative GCS score was 8.04±3.18, and the average GCS score of patients was 11.13±3.11 one week after surgery. There were statistically significant differences in preoperative and postoperative GCS score. Z=4.036, **P < 0.01.
表 1 患者基本信息
Table 1. General information of the patients
General Information Value (n=24) Location of cerebral hemorrhage (n) Supratentorial hematoma 17 Subtentorial hematoma 7 Gender (n) Male 20 Female 4 Age (years, Mean±SD) 52.71±10.08 Preoperative hematoma volume(mL, Mean±SD) 29.35±17.77 Postoperative hematoma volume(mL, Mean±SD) 8.81±8.75 Preoperative GCS score (Mean±SD) 8.04±3.18 Postoperative GCS score (Mean±SD) 11.13±3.11 Complication (n) Recurrent hemorrhage 0 Incision infection 0 Intracranial infection 0 GCS: Glasgow coma scale.  下载: 导出CSV
下载: 导出CSV
-
[1] Morgenstern LB, Rd JH, Anderson C, et al. Guidelines for the management of spontaneous intracerebral hemorrhage: a guideline for healthcare professionals from the American heart association/American stroke association[J]. Stroke, 2015, 46(7): 2032-60. doi: 10.1161/STR.0000000000000069 [2] Krishnamurthi RV, Feigin VL, Forouzanfar MH, et al. Global and regional burden of first-ever ischaemic and haemorrhagic stroke during 1990-2010: findings from the Global Burden of Disease Study 2010[J]. Lancet Glob Health, 2013, 1(5): e259-81. doi: 10.1016/S2214-109X(13)70089-5 [3] 赵继宗, 周定标, 周良辅, 等. 2464例高血压脑出血外科治疗多中心单盲研究[J]. 中华医学杂志, 2005, 85(32): 2238-42. doi: 10.3760/j:issn:0376-2491.2005.32.004 [4] Fernandes H, Gregson B, Siddique S, et al. Surgery in intracerebral hemorrhage: the uncertainty continues[J]. Stroke J Am Heart Assoc, 2000, 31: 2511-6. [5] 张帆, 游潮. 高血压脑出血手术治疗的研究进展[J]. 中国脑血管病杂志, 2010, 7(4): 210-4. doi: 10.3969/j.issn.1672-5921.2010.04.011 [6] Choi JW, Lee JY, Phi JH, et al. Stricter indications are recommended for fenestration surgery in intracranial arachnoid cysts of children[J]. Childs Nerv Syst, 2015, 31(1): 77-86. doi: 10.1007/s00381-014-2525-1 [7] 侯晓帅, 孙健永, 孙树杰, 等. 一种基于图像3D MPR的脑出血定位方法研究[J]. 中国数字医学, 2016, 11(8): 97-100. https://www.cnki.com.cn/Article/CJFDTOTAL-YISZ201608044.htm [8] 徐兴华, 陈晓雷, 张军, 等. 多田公式计算脑内血肿体积的准确性和可靠性[J]. 中国神经精神疾病杂志, 2015, 41(2): 87-91. https://www.cnki.com.cn/Article/CJFDTOTAL-ZSJJ201502006.htm [9] Kothari RU, Brott T, Broderick JP, et al. The ABCs of measuring intracerebral hemorrhage volumes[J]. Stroke, 1996, 27(8): 1304-5. doi: 10.1161/01.STR.27.8.1304 [10] 魏大年, 刘铁坚, 张冠华, 等. 脑内血肿穿刺引流简易定位法: "两点两线法"[J]. 中华神经医学杂志, 2017, 16(1): 70-4. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGLC201811016.htm [11] Liu YQ, Song ZH, Liu CY, et al. A novel surgical technique for spontaneous intracerebral hematoma evacuation[J]. Neurosurg Rev, 2021, 44(2): 925-34. doi: 10.1007/s10143-020-01252-z [12] 徐昌浓, 张洪标, 曾维余, 等. MSCT重建技术在薄层急性硬膜下血肿中的应用价值[J]. 现代医用影像学, 2020, 29(2): 202-5. https://www.cnki.com.cn/Article/CJFDTOTAL-XDYY202002003.htm [13] 杨志华. 微创首次抽吸量与再出血常见原因分析[J]. 中外健康文摘, 2013(24): 83-4. [14] 董俊峰. 脑出血微创术抽吸力量与术后再出血关系研究[J]. 河南科技大学学报: 医学版, 2011, 29(2): 105-7. https://www.cnki.com.cn/Article/CJFDTOTAL-LYYZ201102010.htm [15] Zhou HG, Zhang Y, Liu L, et al. Minimally invasive stereotactic puncture and thrombolysis therapy improves long-term outcome after acute intracerebral hemorrhage[J]. J Neurol, 2011, 258(4): 661-9. [16] Fam MD, Hanley D, Stadnik A, et al. Surgical performance in minimally invasive surgery plus recombinant tissue plasminogen activator for intracerebral hemorrhage evacuation phase Ⅲ clinical trial[J]. Neurosurgery, 2017, 81(5): 860-6. [17] Li YQ, Yang RX, Li ZH, et al. Urokinase vs tissue-type plasminogen activator for thrombolytic evacuation of spontaneous intracerebral hemorrhage in basal Ganglia[J]. Front Neurol, 2017, 8: 371. [18] 郭卫东. 高血压脑出血立体定向手术与内科保守治疗疗效对比分析[J]. 中华高血压杂志, 2011, 19(12): 1200. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGGZ201112043.htm [19] Fried HI, Nathan BR, et al. The insertion and management of external ventricular drains: an evidence-based consensus statement[J]. Neurocrit Care, 2016, 24(1): 61-81. [20] 毛群, 勾俊龙, 刘宗惠. 外科治疗脑出血: 回顾与展望[J]. 国外医学神经病学神经外科学分册, 2003, 30(5): 420-3. https://xuewen.cnki.net/CCND-CFNB202010270050.html [21] Hanley DF, Thompson RE, Muschelli J, et al. Safety and efficacy of minimally invasive surgery plus alteplase in intracerebral haemorrhage evacuation (MISTIE): a randomised, controlled, open-label, phase 2 trial[J]. Lancet Neurol, 2016, 15(12): 1228-37. [22] Hinson HE, Melnychuk E, Muschelli J, et al. Drainage efficiency with dual versus single catheters in severe intraventricular hemorrhage[J]. Neurocrit Care, 2012, 16(3): 399-405. [23] Barnes B, Hanley DF, Carhuapoma JR. Minimally invasive surgery for intracerebral haemorrhage[J]. Curr Opin Crit Care, 2014, 20(2): 148-52. [24] 杨术真, 李拴德, 杨喜民, 等. 采用CT影像结合徒手体表定位经皮颅骨锥孔引流治疗高血压脑出血116例[J]. 中国危重病急救医学, 2000(5): 311-2. https://www.cnki.com.cn/Article/CJFDTOTAL-ZWZB200005031.htm [25] Brown RA. A stereotactic head frame for use with CT body scanners[J]. Investig Radiol, 1979, 14(4): 300-4. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 146
- HTML全文浏览量: 44
- PDF下载量: 21
- 被引次数: 0