



Predictive value of right heart contrast echocardiography combined with score for the targeting of atrial fibrillation in cardiac embolism
-
摘要:
目的 探究右心声学造影联合房颤鉴别评分(STAF)对心源性脑梗死(CE)预测价值。 方法 回顾性分析2017年8月~2021年8月医院收治149例CE患者及93例非心源性脑梗死(NCE)患者资料,分别作为CE组与NCE组。患者均接受右心声学造影及STAF,比较两组患者右心声学造影结果及STAF,分析右心声学造影联合STAF对CE的预测价值;CE患者随访1年,评估CE患者预后情况,分析CE患者预后影响因素。 结果 CE组患者1级+2级+3级右向左分流分级、卵圆孔未闭阳性率、卵圆孔长径、分流口内径均高于NCE组(P < 0.05);CE组患者STAF高于NCE组患者(P < 0.05);ROC曲线显示右向左分流分级、卵圆孔未闭阳性率、卵圆孔长径、分流口内径、STAF用于CE预测曲线下面积分别为0.582、0.570、0.679、0.808、0.750,各指标联合AUC值为0.905;单因素与多元Logistic回归分析显示房颤、总胆固醇、纤维蛋白原不是CE患者预后影响因素(P > 0.05),入院时NIHSS评分、卵圆孔未闭阳性率、卵圆孔长径、STAF是CE患者预后影响因素(P < 0.05)。 结论 右心声学造影联合STAF有助于提高心源性脑梗死预测价值。 Abstract:Objective To investigate the predictive value of right heart contrast echocardiography combined with the score for the targeting of atrial fibrillation (STAF) in cardiac embolism (CE). Methods We retrospectively analyzed the data of 149 patients with CE (CE group) and 93 patients with non-cardiac embolism (NCE group) who were admitted to the hospital from August 2017 to August 2021. The results of right heart contrast echocardiography and STAF scores in the two groups were compared. The predictive value of right heart contrast echocardiography combined with STAF in CE was analyzed. Patients with CE were followed up for 1 year to evaluate the prognosis. The prognostic factors in patients with CE were analyzed. Results The proportions of patients with grade 1, grade 2 and grade 3 right-to-left shunt, the positive rate of patent foramen ovale, long diameter of foramen ovale, and diameter of shunt orifice in CE group were higher/larger than those in NCE group (P < 0.05). The STAF score of CE group was higher than that of NCE group (P < 0.05). ROC curve analysis showed that the area under the curve values of right-to-left shunt grade, positive rate of patent foramen ovale, long diameter of foramen ovale, diameter of shunt orifice, STAF and their combination to predict CE were 0.582, 0.570, 0.679, 0.808, 0.750 and 0.905. Univariate analysis and multivariate logistic regression analysis found that the NIHSS score at admission, the positive rate of patent foramen ovale, long diameter of foramen ovale, and STAF were prognostic factors in patients with CE (P < 0.05). Conclusion Right heart contrast echocardiography combined with STAF is beneficial to predict CE. -

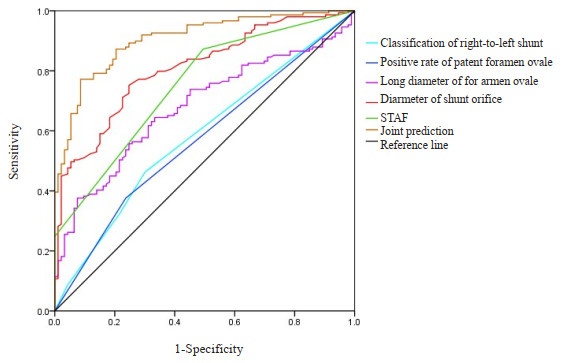
图 1 右心声学造影检查结果联合STAF对CE预测价值分析ROC曲线
Figure 1. ROC curves of right heart contrast echocardiography results combined with STAF for predicting CE.
表 1 两组患者一般资料对比
Table 1. Comparison of general data between the two groups (Mean±SD)
Group Gender (n) Age (year) Course of disease (h) NIHSS score (point) Male Female CE group (n=149) 84 65 58.64±13.69 2.18±0.41 10.75±2.86 NCE group (n=93) 45 48 60.13±13.75 2.29±0.57 10.94±2.65 t/χ2 1.468 0.822 1.742 0.517 P 0.226 0.412 0.083 0.606 CE: Cardiac embolism; NCE: Non-cardiac embolism; NIHSS: National institute of health stroke scale.  下载: 导出CSV
下载: 导出CSV
表 2 两组患者右心声学造影检查结果比较
Table 2. Comparison of right heart contrast echocardiography results between the two groups.
Item CE group (n=149) NCE group (n=93) P Classification of right-to-left shunt[n (%)] Grade 0 80(53.69) 65(69.89) Grade 1 21(14.09) 8(8.60) Grade 2 35(23.49) 16(17.20) Grade 3 13(8.72) 4(4.30) Grade 1+grade 2+ grade 3 69(46.31) 28(30.11) 0.012 Positive rate of patent foramen ovale 76(51.01) 32(34.41) 0.012 Long diameter of foramen ovale (mm, Mean±SD) 12.13±2.89 10.26±1.97 < 0.001 Diameter of shunt orifice (mm, Mean±SD) 1.44±0.42 1.03±0.31 < 0.001
下载: 导出CSV
表 3 右心声学造影检查结果联合STAF对CE预测价值分析
Table 3. Predictive value of right heart contrast echocardiography combined with STAF for CE
Item Cut-off value AUC Sensitivity (%) Specificity (%) 95% CI P Classification of right-to-left shunt - 0.582 46.3 69.9 0.509-0.655 0.032 Positive rate of patent foramen ovale - 0.570 37.6 76.3 0.496-0.643 0.068 Long diameter of foramen ovale 11.34 mm 0.679 64.4 66.7 0.612-0.745 < 0.001 Diameter of shunt orifice 1.15 mm 0.808 75.2 75.3 0.754-0.862 < 0.001 STAF 2 0.750 87.2 50.6 0.689-0.812 < 0.001 Joint prediction - 0.905 77.2 91.4 0.868-0.942 < 0.001 STAF: Score for the targeting of atrial fibrillation; AUC: Area under curve.
下载: 导出CSV
表 4 CE患者预后单因素分析
Table 4. Univariate analysis of the prognosis of patients with CE (Mean±SD)
Item In total
(n=149)Good prognosis group
(n=117)Poor prognosis group
(n=32)t/χ2 P Gender (n) 0.149 0.699 Male 84 65 19 Female 65 52 13 Age(year) 58.64±13.69 58.53±13.19 59.04±15.61 0.187 0.852 Atrial fibrillation (n) 25 15 10 6.112 0.013 Drinking history (n) 36 28 8 0.016 0.900 Smoking history (n) 47 39 8 0.808 0.369 Diabetes (n) 38 28 10 0.708 0.400 Course of disease (h) 2.19±0.39 2.14±0.48 0.568 0.571 NIHSS score at admission (point) 10.31±2.34 12.36±3.89 3.750 < 0.001 Creatine kinase isoenzyme (U/L) 4.26±1.72 4.38±1.53 0.358 0.721 High-density lipoprotein (mmol/L) 1.09±0.29 1.13±0.31 0.681 0.497 Triglyceride (mmol/L) 1.89±0.34 1.81±0.36 1.165 0.246 Low density lipoprotein (mmol/L) 2.38±0.62 2.49±0.67 0.874 0.384 Total cholesterol (mmol/L) 4.29±0.89 4.67±0.84 2.165 0.032 Systolic pressure (mmHg) 149.65±21.16 154.71±19.62 1.217 0.226 Fasting blood glucose (mmol/L) 5.84±1.29 6.15±1.41 1.181 0.240 Diastolic blood pressure (mmHg) 92.14±10.47 91.53±11.65 0.285 0.776 Fibrinogen (g/L) 3.07±0.76 3.46±0.71 2.608 0.010 D-dimer (mg/L) 0.58±0.16 0.59±0.15 0.317 0.751 Homocysteine (μmol/L) 10.12±2.35 9.86±2.54 0.545 0.587 Classification of right-to-left shunt (n) 1.093 0.779 Grade 0 80 62 18 Grade 1 21 16 5 Grade 2 35 28 7 Grade 3 13 10 5 Positive rate of patent foramen ovale (n) 69 47 22 8.254 0.004 Long diameter of foramen ovale (mm) 11.58±2.24 14.14±3.97 4.755 < 0.001 Diameter of shunt orifice (mm) 1.41±0.41 1.55±0.44 1.677 0.096 STAF (point) 2.03±0.51 2.45±0.62 3.93 < 0.001
下载: 导出CSV
表 5 CE患者预后多因素多元Logistic回归分析
Table 5. Multivariate logistic regression analysis of the prognosis of patients with CE
Item β SE Wald χ2 OR 95% CI P Atrial fibrillation 0.516 0.311 2.753 1.675 0.911-3.082 0.098 NIHSS score at admission 0.408 0.206 3.923 1.504 1.004-2.252 0.048 Total cholesterol 0.486 0.374 1.689 1.626 0.781-3.384 0.194 Fibrinogen 0.428 0.319 1.800 1.534 0.821-2.867 0.180 Positive rate of patent foramen ovale 0.626 0.245 6.529 1.870 1.157-3.023 0.011 Long diameter of foramen ovale 0.573 0.226 6.428 1.774 1.139-2.762 0.012 STAF 0.517 0.232 4.966 1.677 1.064-2.642 0.026
下载: 导出CSV
-
[1] Wu B, Wang Y, Li W, et al. The effect of rosuvastatin on cardiogenic cerebral infarction[J]. Am J Transl Res, 2021, 13(8): 9444-50. [2] Ding HJ, Ma C, Ye FP, et al. Bridging therapy and direct mechanical thrombectomy in the treatment of cardiogenic cerebral infarction with anterior circulation macrovascular occlusion[J]. World J Clin Cases, 2021, 9(27): 8051-60. doi: 10.12998/wjcc.v9.i27.8051 [3] Suzuki A, Tsubakino S, Fujii H. Motor function and activities of daily living recovery after cardiogenic internal carotid artery infarction: a retrospective cohort study[J]. J Stroke Cerebrovasc Dis, 2021, 30(6): 105734. doi: 10.1016/j.jstrokecerebrovasdis.2021.105734 [4] Inoue N, Morikawa S. Unusual case of cerebral embolism after initiation of selexipag for sarcoidosis-related pulmonary hypertension: a case report[J]. Radiol Case Rep, 2022, 17(9): 3009-14. doi: 10.1016/j.radcr.2022.05.064 [5] Nakayama R, Takaya Y, Akagi T, et al. Identification of high-risk patent foramen ovale associated with cryptogenic stroke: development of a scoring system[J]. J Am Soc Echocardiogr, 2019, 32(7): 811-6. doi: 10.1016/j.echo.2019.03.021 [6] Miton N, Godart F, Milani G, et al. Patent foramen ovale closure in children without cardiopathy: child-PFO study[J]. Arch Cardiovasc Dis, 2020, 113(8/9): 513-24. [7] Chen XD, Luo WL, Li JM, et al. Diagnostic accuracy of STAF, LADS, and iPAB scores for predicting paroxysmal atrial fibrillation in patients with acute cerebral infarction[J]. Clin Cardiol, 2018, 41(12): 1507-12. doi: 10.1002/clc.23080 [8] 安娜, 邓元友, 武联军. iPAB和STAF评分系统对急性缺血性脑卒中患者发生阵发性心房颤动的预测价值[J]. 中国医药, 2019, 14(3): 357-61. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGYG201903010.htm [9] 中华医学会神经病学分会脑血管病学组急性缺血性脑卒中诊治指南撰写组. 中国急性缺血性脑卒中诊治指南2010[J]. 中国全科医学, 2011(35): 4013-7. doi: 10.3969/j.issn.1007-9572.2011.35.004 [10] 冯坤. 3种不同手振激活声学造影剂在经胸超声心动图右心声学造影及经颅脑血管微泡试验中应用的对比研究[D]. 泸州: 西南医科大学, 2018. [11] 梅文丽. 伴发卵圆孔未闭的隐源性卒中的神经影像学特征分析[D]. 郑州: 郑州大学, 2017. [12] Ozaydin Goksu E, Yuksel B, Esin M, et al. The value of STAF (score for the targeting of atrial fibrillation) in patients with cryptogenic embolic stroke[J]. Arch Neuropsychiatr, 2017: 119-22. [13] 李达, 李利, 刘晓霞, 等. cTTE+隐源性卒中患者临床特征及影像学分析[J]. 中风与神经疾病杂志, 2022, 39(7): 585-90. https://www.cnki.com.cn/Article/CJFDTOTAL-ZFSJ202207002.htm [14] 蔡珍飞, 吴肖萍, 曹丹. 2017年台州地区急性脑梗死发生的流行特征[J]. 实用预防医学, 2019, 26(10): 1247-50. https://www.cnki.com.cn/Article/CJFDTOTAL-SYYY201910026.htm [15] Umemura T, Hachisuka K, Miyachi H, et al. Clinical outcomes of cerebral infarction in nonagenarians compared among four age groups[J]. Neurol Sci, 2020, 41(9): 2471-6. doi: 10.1007/s10072-020-04348-y [16] Leitman M, Blondheim DS, Sabetay S, et al. Diagnosis of patent foramen ovale using maximum intensity T-projection imaging[J]. Int J Cardiovasc Imaging, 2021, 37(4): 1343-8. doi: 10.1007/s10554-020-02123-w [17] 赵志宏, 宋湘, 王赛华, 等. 卵圆孔未闭伴心房颤动患者行左心耳联合卵圆孔未闭封堵安全性与有效性初探[J]. 中华心血管病杂志, 2022, 50(3): 257-62. doi: 10.3760/cma.j.cn112148-20211214-01073 [18] Zhu Y, Zhang J, Huang B, et al. Impact of patent foramen ovale anatomic features on right-to-left shunt in patients with cryptogenic stroke[J]. Ultrasound Med Biol, 2021, 47(5): 1289-98. doi: 10.1016/j.ultrasmedbio.2021.01.004 [19] 王一茹, 邓玉姣, 阳开秀, 等. 卵圆孔未闭经胸超声心动图声学造影及经食管超声心动图的单中心诊断数据分析[J]. 中华医学超声杂志: 电子版, 2020, 17(6): 546-51. https://www.cnki.com.cn/Article/CJFDTOTAL-ZHCD202006014.htm [20] 席芬, 杨毓雯, 杜微云. 经胸超声心动图及右心声学造影对成人卵圆孔未闭诊断效能的比较[J]. 中国超声医学杂志, 2020, 36(7): 617-20. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGCY202007014.htm [21] 傅庆华, 何晋, 余翔, 等. 不同辅助方式下经胸右心声学造影对卵圆孔未闭诊断价值的比较[J]. 广东医学, 2021, 42(10): 1219-23. https://www.cnki.com.cn/Article/CJFDTOTAL-GAYX202110017.htm [22] 王凤霞, 许中兴, 陶静, 等. 经胸超声心动图右心声学造影在"反常栓塞" 卵圆孔未闭封堵治疗中的临床应用[J]. 心脑血管病防治, 2021, 21(5): 476-9. https://www.cnki.com.cn/Article/CJFDTOTAL-XXFZ202105016.htm [23] Barigye SJ, de la Vega JMG, Castillo-Garit JA. Undersampling: case studies of flaviviral inhibitory activities[J]. J Comput Aided Mol Des, 2019, 33(11): 997-1008. [24] 鲁桃, 吕哲, 陆小林, 等. 心肌肌钙蛋白I升高和STAF评分对心源性脑梗死的预测价值[J]. 中国神经精神疾病杂志, 2019, 45(6): 331-5. https://www.cnki.com.cn/Article/CJFDTOTAL-ZSJJ201906004.htm [25] 高伟芳, 陈蓓蕾, 吉莉. 颈部动脉夹层继发前循环脑梗死的临床特征及预后分析[J]. 中风与神经疾病杂志, 2021, 38(8): 696-700. https://www.cnki.com.cn/Article/CJFDTOTAL-ZFSJ202108006.htm [26] Gui X, Wang L, Wu C, et al. Prognosis of subtypes of acute large artery atherosclerotic cerebral infarction by evaluation of established collateral circulation[J]. J Stroke Cerebrovasc Dis, 2020, 29(11): 105232-48. -




 点击查看大图
点击查看大图
计量
- 文章访问数: 126
- HTML全文浏览量: 120
- PDF下载量: 5
- 被引次数: 0