



Dual-energy CT multiple quantitative parameters can evaluate the proliferative activity of high-grade serous ovarian carcinoma
-
摘要:
目的 探讨双能量CT多定量参数无创评估卵巢高级别浆液性癌肿瘤细胞增殖能力的价值。 方法 回顾性收集2021年6月~2023年1月盐城市第一人民医院66例经手术证实的连续性卵巢高级别浆液性癌病例,所有患者术前2周内均行能谱CT平扫及增强扫描,术后所有肿瘤组织病理标本切片行Ki-67免疫组织化学染色,根据术后病理分为Ki-67高表达组(n=34)及Ki-67低表达组(n=32);由2位观察者分别独立测量病灶动脉期及静脉期40~90 keV单能量CT值、碘浓度,计算标准化碘浓度及能谱曲线斜率(K40-90 keV);采用组内相关系数检验2位测量者测量参数之间相关性及一致性的程度;比较两组之间各参数的差异,对差异有统计学意义的参数采用ROC曲线分析诊断效能,并分析差异有统计学意义的参数与Ki-67表达的相关性。 结果 2位测量者对动脉期、静脉期两组间测得的各参数一致性较好,组内相关系数均大于0.75;低表达组动脉期、静脉期40~70 keV单能量CT值、K40-90 keV、碘浓度、标准化碘浓度均低于Ki-67高表达组(P < 0.05),ROC曲线分析显示动脉期K40-90 keV诊断效能最高,曲线下面积为0.913,敏感度为91.2%,特异性为87.5%,阈值为0.95,上述参数与Ki-67表达均有相关性,以动脉期K40-90 keV与其的相关系数最高(rs=-0.900,P < 0.001)。 结论 双能量CT多定量参数可无创评估卵巢高级别浆液性癌肿瘤细胞的增殖能力。 Abstract:Objective To explore the value of non-invasive assessment for the proliferative ability of ovarian high-grade serous carcinoma tumor cells using dual-energy CT multiple quantitative parameters. Methods We retrospectively analyzed 66 cases of high-grade serous ovarian carcinoma confirmed by surgery at the First People's Hospital of Yancheng City from June 2021 to January 2023. All patients underwent spectral CT plain and enhanced scans within 2 weeks prior to surgery. After surgery, all tumor tissue pathological specimens were stained with Ki-67 immunohistochemistry. According to postoperative pathological findings, patients were classified into Ki-67 high expression group (n=34) and Ki-67 low expression group (n=32). The measurement of arterial and venous phase single-energy CT values (40-90 keV) and iodine concentration of the lesions were independently conducted by two observers. Normalized iodine concentration and energy spectrum curve slope (K40-90 keV) were calculated. Intra-group correlation coefficient was used to evaluate the consistency and correlation between the measurement parameters of the two observers. The differences in various parameters between the two groups were compared. ROC curves were calculated to evaluate the diagnostic efficacy of the related parameters with statistically significant differences. The correlation between the parameters with statistically significant differences and Ki-67 expression was analyzed. Results Two observers showed good consistency in the measurement of various parameters in the arterial and venous phases, with all the intra-group correlation coefficient was greater than 0.75. The low expression group had lower arterial and venous phase 40-70 keV single-energy CT values, iodine concentration, normalized iodine concentration and K40-90 keV than the high expression group (P < 0.05). ROC curve analysis showed that the diagnostic efficacy of arterial phase K40-90 keV was the highest, with an AUC of 0.913, sensitivity of 91.2%, specificity of 87.5%, and a threshold of 0.95. The above parameters were also correlated with Ki-67 expression, with the highest correlation coefficient observed between arterial phase K40-90keV and Ki-67 (rs=-0.900, P < 0.001). Conclusion Dual-energy CT can non-invasively evaluate the proliferative ability of high-grade serous ovarian carcinoma cells using multiple quantitative parameters. -

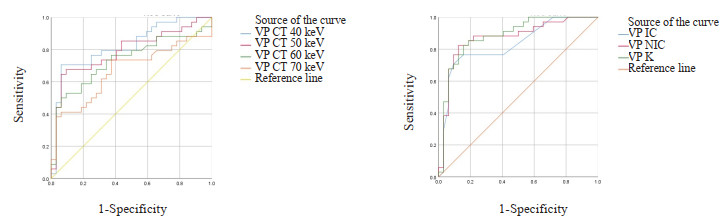
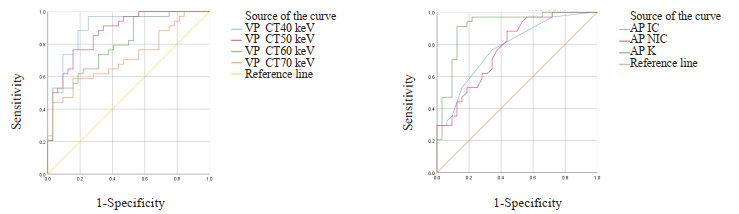
图 1 动脉期双能量各参数鉴别Ki-67表达的ROC曲线
Figure 1. ROC curves of each parameter of dual energy in the arterial phase to identify Ki-67 expression.

图 2 静脉期双能量各参数鉴别Ki-67表达的ROC曲线
Figure 2. ROC curves of each parameter of dual energy in the intravenous phase to identify Ki-67 expression.

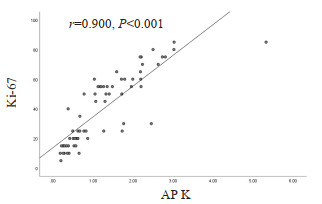
图 3 动脉期K40-90 keV与Ki-67表达的相关性分析散点图
Figure 3. Scatter plot of correlation analysis between K40-90 keV and Ki-67 expression in the arterial phase.

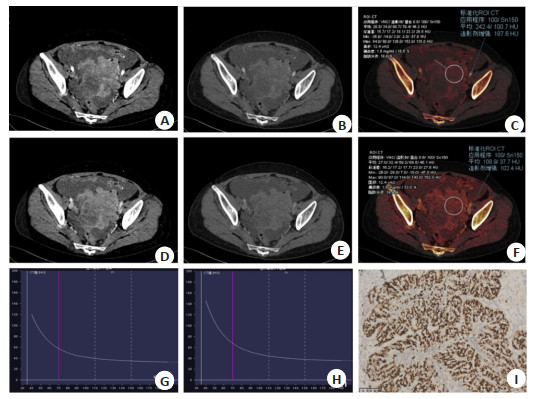
图 4 高表达组患者双能量CT参数测量结果及Ki-67表达图
Figure 4. Results of dual-energy CT parameter measurements and Ki-67 expression maps of patients in the high expression group. Female, 54 years old, HGSOC of the left side, Ki-67 (80%). A-B: Mono-energy CT images (40 keV, 70 keV) in arterial phase; D, E: Mono-energy CT images (40 keV, 70 keV) in venous phase; C, F: Iodine density in arterial and venous phases; G, H: Energy spectrum curve in arterial and venous phases; I: Microscopic yellowish staining of tumor cell nuclei (SP, 10×20), Ki-67 (80%).

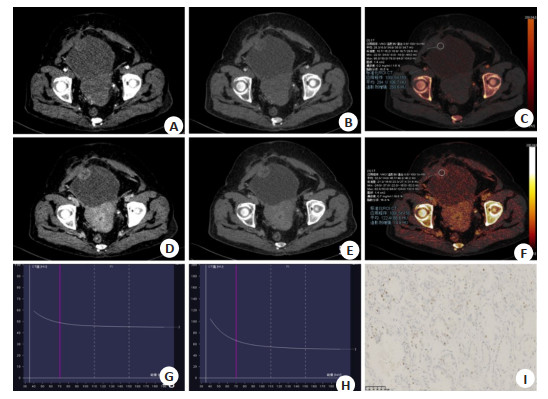
图 5 低表达组患者双能量CT参数测量结果及Ki-67表达图
Figure 5. Dual-energy CT parameter measurements and Ki-67 expression maps of patients in the low expression group. Female, 54 years old, HGSOC of the right side, Ki-67(20%). A, B: Mono-energy CT images (40 keV, 70 keV) in arterial phase; D, E: Mono-energy CT images (40 keV, 70 keV) in venous phase; C, F: Iodine density in arterial and venous phases; G, H: Energy spectrum curve in arterial and venous phases; I: Microscopic yellowish staining of tumor cell nuclei (SP, 10×20), Ki-67 (20%).
表 1 两组患者一般资料对比
Table 1. Comparison of general information between the two groups of patients
Index Ki-67≤30% group(n=32) Ki-67 > 30% group(n=34) χ2/t P Age(year, Mean±SD) 61.19±10.66 58.06±9.31 1.261 0.212 Occurrence site [n(%)] 0.240 0.887 Left 6(50) 6(50) Right 6(54.5) 5(45.5) Duplex 20(46.5) 23(53.5) Clinical symptoms [n(%)] 0.057 0.811 No 16(47.1) 18(52.9) Yes 16(50) 16(50) Maximum diameter of tumor(mm, Mean±SD) 67.28±47.26 85.91±44.72 -1.646 0.105  下载: 导出CSV
下载: 导出CSV
表 2 动脉期2位测量者对Ki-67高、低表达组患者各参数及其一致性检测结果
Table 2. Results of each parameter and concordance test for patients in the Ki-67 high and low expression groups by two observers during the arterial phase (Mean±SD)
Index Ki-67≤30% group (n=32) Ki-67>30% group (n=34) Observer 1 Observer 2 ICC Observer 1 Observer 2 ICC CT40 keV (Hu) 84.43±25.99 83.67±28.01 0.986 147.11±54.23 145.91±56.78 0.992 CT50 keV (Hu) 72.46±16.71 69.36±16.91 0.980 109.18±36.29 106.85±36.67 0.997 CT60 keV (Hu) 64.12±11.33 61.63±11.15 0.973 85.62±25.28 83.12±25.30 0.991 CT70 keV (Hu) 59.05±8.53 56.84±8.46 0.963 71.17±18.30 69.38±18.27 0.994 CT80 keV (Hu) 55.71±7.18 53.79±7.62 0.952 62.02±14.25 59.99±14.29 0.989 CT90 keV (Hu) 53.60±7.10 51.57±7.14 0.959 55.61±11.10 53.47±11.15 0.979 IC (mg/mL) 0.55±0.21 0.57±0.22 0.936 0.89±0.43 0.90±0.44 0.994 NIC (%) 6.30±2.53 6.62±2.52 0.960 9.59±4.50 10.15±4.62 0.956 IC: Iodine concentration; NIC: Normalized iodine concentration; ICC: Interclass correlation coefficient.
下载: 导出CSV
表 3 静脉期2位测量者对Ki-67高、低表达组患者各参数及一致性检测结果
Table 3. Results of each parameter and concordance test for patients in the Ki-67 high and low expression groups by two measurers during the intravenous period (Mean±SD)
Index Ki-67≤30% group (n=32) Ki-67 > group 30% group (n=34) Observer 1 Observer 2 ICC Observer 1 Observer 2 ICC CT40 keV (Hu) 139.70±41.48 134.38±38.50 0.974 202.03±64.95 198.77±63.52 0.994 CT50 keV (Hu) 108.64±24.48 102.82±24.26 0.969 144.93±41.85 138.73±41.85 0.989 CT60 keV (Hu) 88.82±15.37 83.62±15.37 0.925 110.40±29.11 104.20±29.11 0.978 CT70 keV (Hu) 78.03±10.43 71.83±10.44 0.850 88.98±21.36 82.78±21.37 0.960 CT80 keV (Hu) 69.43±8.01 65.23±8.00 0.879 74.11±16.50 69.91±16.51 0.969 CT90 keV (Hu) 63.67±6.93 60.67±6.92 0.914 64.12±13.26 61.12±13.25 0.975 IC (mg/mL) 1.38±0.27 1.21±0.26 0.808 1.78±0.31 1.59±0.31 0.834 NIC (%) 24.06±5.20 21.99±5.13 0.921 34.45±6.72 32.37±6.85 0.950
下载: 导出CSV
表 4 动脉期两组患者双能量CT各参数
Table 4. Each parameter of dual-energy CT in two groups of patients in arterial phase (Mean±SD)
Index Ki-67≤ 30% group (n=32) Ki-67 > 30% group (n=34) t P CT40 keV (Hu) 84.05±26.93 146.52±55.41 5.766 < 0.001 CT50 keV (Hu) 70.92±16.79 108.03±36.48 5.254 < 0.001 CT60 keV (Hu) 62.89±11.23 84.41±25.3 4.415 < 0.001 CT70 keV (Hu) 57.95±8.48 70.28±18.28 3.477 0.001 CT80 keV (Hu) 54.75±7.37 61.01±14.27 2.216 0.130 CT90 keV (Hu) 52.59±7.12 54.54±11.12 0.844 0.402 K40-90 keV 0.63±0.51 1.84±0.92 6.55 < 0.001 IC (mg/mL) 0.56±0.22 0.89±0.44 3.890 < 0.001 NIC (%) 6.45±2.51 9.80±4.47 3.704 < 0.001
下载: 导出CSV
表 5 静脉期两组患者双能量CT各参数
Table 5. Each parameter of dual-energy CT in two groups of patients in venous phase (Mean±SD)
Index Ki-67≤30% group (n=32) Ki-67 > 30% group (n=34) t P CT40 keV (Hu) 137.04±39.84 200.40±64.17 4.78 < 0.001 CT50 keV (Hu) 105.73±24.35 141.83±41.86 4.24 < 0.001 CT60 keV (Hu) 86.72±15.37 107.30±29.11 3.55 < 0.001 CT70 keV (Hu) 74.93±10.44 85.88±21.36 2.61 0.011 CT80 keV (Hu) 67.33±8.01 72.01±16.50 1.45 0.151 CT90 keV (Hu) 62.18±6.93 62.62±13.26 0.16 0.867 K40-90 keV 1.49±0.76 2.75±1.05 5.54 < 0.001 IC (mg/mL) 1.30±0.27 1.69±0.31 5.38 < 0.001 NIC (%) 23.03±5.16 33.41±6.78 6.96 < 0.001
下载: 导出CSV
表 6 动脉期双能量CT各参数对HGSOC患者Ki-67表达诊断效能分析
Table 6. Analysis of diagnostic efficacy of various parameters of arterial phase dual-energy CT on Ki-67 expression in patients with HGSOC.
Index AUC Sensitivity (%) Specificity (%) Threshold 95% CI CT40 keV (Hu) 0.903 97.1 75.0 90.96 0.829, 0.978 CT50 keV (Hu) 0.871 76.5 84.4 82.02 0.788, 0.955 CT60 keV (Hu) 0.802 52.9 96.9 78.78 0.699, 0.906 CT70 keV (Hu) 0.719 58.8 84.4 65.53 0.595, 0.842 K40-90 keV 0.913 91.2 87.5 0.95 0.838, 0.987 IC (mg/mL) 0.781 76.5 65.6 0.55 0.671, 0.890 NIC (%) 0.776 88.2 56.2 5.85 0.665, 0.886
下载: 导出CSV
表 7 静脉期双能量CT各参数对HGSOC患者Ki-67表达诊断效能分析
Table 7. Analysis of the diagnostic efficacy of each parameter of intravenous phase dual-energy CT on Ki-67 expression in HGSOC patients.
Index AUC Sensitivity (%) Specificity (%) Threshold 95% CI CT40 keV (Hu) 0.823 70.6 93.7 158.49 0.719, 0.926 CT50 keV (Hu) 0.790 64.7 93.7 121.30 0.677, 0.904 CT60 keV (Hu) 0.734 50.0 93.7 101.52 0.609, 0.859 CT70 keV (Hu) 0.667 73.5 62.5 70.05 0.533, 0.801 K40-90 keV 0.882 82.4 84.4 1.74 0.798, 0.962 IC (mg/mL) 0.827 70.6 90.6 1.55 0.724, 0.930 NIC (%) 0.869 82.4 87.5 24.80 0.776, 0.962
下载: 导出CSV
表 8 动、静脉期双能量CT各参数与Ki-67表达的Spearman相关性分析
Table 8. Spearman correlation analysis between each parameter of dual energy CT and Ki-67 expression in the arterial and venous phase
Index Arterial phase Venous phase rs P rs P CT40 keV 0.890 < 0.001 0.688 < 0.001 CT50 keV 0.850 < 0.001 0.603 < 0.001 CT60 keV 0.763 < 0.001 0.492 < 0.001 CT70 keV 0.622 < 0.001 0.343 < 0.001 K40-90 keV 0.900 < 0.001 0.759 < 0.001 IC 0.739 < 0.001 0.683 < 0.001 NIC 0.779 < 0.001 0.750 < 0.001
下载: 导出CSV
-
[1] Singh N, McCluggage WG, Gilks CB. High-grade serous carcinoma of tubo-ovarian origin: recent developments[J]. Histopathology, 2017, 71(3): 339-56. doi: 10.1111/his.13248 [2] Jiang XY, Tang HJ, Chen TH. Epidemiology of gynecologic cancers in China[J]. J Gynecol Oncol, 2018, 29(1): e7. doi: 10.3802/jgo.2018.29.e7 [3] Gerdes J, Lemke H, Baisch H, et al. Cell cycle analysis of a cell proliferation-associated human nuclear antigen defined by the monoclonal antibody Ki-67[J]. J Immunol, 1984, 133(4): 1710-5. doi: 10.4049/jimmunol.133.4.1710 [4] Varghese JR, Gurusamy DS, Kalyanasundaram S, et al. Role of podoplanin, E-cadherin, Ki-67 in the dissemination of tumor cells in ovarian surface epithelial carcinoma-An immunohistochemical study[J]. Ann Diagn Pathol, 2022, 60: 151984. doi: 10.1016/j.anndiagpath.2022.151984 [5] Qiu DM, Cai WQ, Zhang ZQ, et al. High Ki-67 expression is significantly associated with poor prognosis of ovarian cancer patients: evidence from a meta-analysis[J]. Arch Gynecol Obstet, 2019, 299(5): 1415-27. doi: 10.1007/s00404-019-05082-3 [6] Deng Y, Chen C, Hua MH, et al. Annexin A2 plays a critical role in epithelial ovarian cancer[J]. Arch Gynecol Obstet, 2015, 292(1): 175-82. doi: 10.1007/s00404-014-3598-5 [7] Ellis MJ, Suman VJ, Hoog J, et al. Ki67 proliferation index as a tool for chemotherapy decisions during and after neoadjuvant aromatase inhibitor treatment of breast cancer: results from the American college of surgeons oncology group Z1031 trial (alliance)[J]. J Clin Oncol, 2017, 35(10): 1061-9. doi: 10.1200/JCO.2016.69.4406 [8] Zhang Y, Cheng JJ, Hua XL, et al. Can spectral CT imaging improve the differentiation between malignant and benign solitary pulmonary nodules?[J]. PLoS One, 2016, 11(2): e0147537. doi: 10.1371/journal.pone.0147537 [9] Han X, Li B, Sun M, et al. Application of contrast-enhanced dual-energy spectral CT for differentiating borderline from malignant epithelial ovarian tumours[J]. Clin Radiol, 2021, 76(8): 585-92. doi: 10.1016/j.crad.2021.04.004 [10] 张于凤, 李辉, 李晶晶, 等. 能谱CT多模态参数联合临床参数对胃间质瘤Ki-67的预测价值[J]. 分子影像学杂志, 2022, 45(5): 688-92. doi: 10.12122/j.issn.1674-4500.2022.05.11 [11] 方梦佳, 刘威武, 杨丹, 等. 磁共振弥散加权成像不同模型预测卵巢癌Ki-67表达的研究进展[J]. 国际老年医学杂志, 2021, 42(5): 301-4. https://www.cnki.com.cn/Article/CJFDTOTAL-GWLL202105013.htm [12] Stewart SL, Harewood R, Matz M, et al. Disparities in ovarian cancer survival in the United States (2001-2009): findings from the CONCORD-2 study[J]. Cancer, 2017, 123: 5138-59. doi: 10.1002/cncr.31027 [13] Berek JS, Renz M, Kehoe S, et al. Cancer of the ovary, fallopian tube, and peritoneum: 2021 update[J]. Int J Gynaecol Obstet, 2021, 155(Suppl 1): 61-85. [14] Torre LA, Trabert B, DeSantis CE, et al. Ovarian cancer statistics, 2018[J]. CA A Cancer J Clin, 2018, 68(4): 284-96. doi: 10.3322/caac.21456 [15] Kaya R, Takanashi H, Nakajima A, et al. Prognostic significance of Ki67 during neoadjuvant chemotherapy in primary unresectable ovarian cancer[J]. J Obstet And Gynaecol, 2021, 47(11): 3979-89. doi: 10.1111/jog.14981 [16] Heayn M, Skvarca LB, Zhu L, et al. Impact of ki-67 labeling index on prognostic significance of the chemotherapy response score in women with tubo-ovarian cancer treated with neoadjuvant chemotherapy[J]. Int J Gynecol Pathol, 2020, 40(3): 278-85. [17] Wortman JR, Sodickson AD. Pearls, pitfalls, and problems in dual-energy computed tomography imaging of the body[J]. Radiol Clin N Am, 2018, 56(4): 625-40. doi: 10.1016/j.rcl.2018.03.007 [18] Deng K, Li W, Wang JJ, et al. The pilot study of dual-energy CT gemstone spectral imaging on the image quality of hand tendons[J]. Clin Imaging, 2013, 37(5): 930-3. doi: 10.1016/j.clinimag.2013.01.008 [19] 杨帆, 潘雪琳, 陈洁, 等. 双能量CT定量参数预测乳腺浸润性导管癌Ki-67表达的可行性探讨[J]. 四川医学, 2021, 42(10): 1037-41. https://www.cnki.com.cn/Article/CJFDTOTAL-SCYX202110014.htm [20] Ju Y, Liu A, Dong Y, et al. The value of nonenhanced single-source dual-energy CT for differentiating metastases from adenoma in adrenal glands[J]. Acad Radiol, 2015, 22(7): 834-9. doi: 10.1016/j.acra.2015.03.004 [21] Yang CB, He TP, Duan HF, et al. Quantitative assessment of the degree of differentiation in colon cancer with dual-energy spectral CT[J]. Abdom Radiol, 2017, 42(11): 2591-6. doi: 10.1007/s00261-017-1176-6 [22] Elsherif SB, Zheng S, Ganeshan D, et al. Does dual-energy CT differentiate benign and malignant ovarian tumours?[J]. Clin Radiol, 2020, 75(8): 606-14. doi: 10.1016/j.crad.2020.03.006 [23] 于利智. 宝石能谱CT检查卵巢肿瘤的临床价值分析[J]. 医学影像学杂志, 2019, 29(7): 1176-80. https://www.cnki.com.cn/Article/CJFDTOTAL-XYXZ201907033.htm [24] 姜明瀚, 黄松, 盛伟华, 等. 双能CT鉴别诊断卵巢良性和恶性肿瘤的价值[J]. 海南医学, 2020, 31(24): 3214-8. https://www.cnki.com.cn/Article/CJFDTOTAL-HAIN202024025.htm -

 点击查看大图
点击查看大图
计量
- 文章访问数: 75
- HTML全文浏览量: 94
- PDF下载量: 7
- 被引次数: 0