



Imaging and clinical features of heptic portal vein gas
-
摘要:
目的 探讨肝脏门静脉积气(HPVG)的临床及影像学特征。 方法 回顾性分析10例HPVG患者的资料,结合文献对其临床特征、影像学特征、治疗及预后进行总结。 结果 10例患者中,以急性消化道症状起病7例,发热5例。存在肾功能不全、维持性血透等相关病史3例,高血压病8例,外科手术史6例。临床诊断中肠梗阻5例,重症感染、感染性休克6例。10例患者仅3例存活。采取手术治疗的2例患者均确诊为肠坏死。HPVG量无论多少均以门静脉左支分布为著;10例中脾静脉、肠系膜上静脉积气7例,肠壁下积气9例;局部肠壁水肿7例,肠梗阻5例,消化道穿孔3例。在5例增强扫描病例中,肠系膜上动脉血栓2例。 结论 HPVG病例中合并肠壁下积气的发生率较高,临床应重视HPVG及相关影像特征的识别,从而对患者进行及时干预。 Abstract:Objective To investigate the imaging and clinical features of hepatic portal vein gas (HPVG). Methods The data of 10 HPVG patients in the Second People's Hospital of Lianyungang, Zhongda Hospital Southeast University from June 2012 to April 2020 were analyzed retrospectively. The imaging and clinical features, treatment and prognosis were summarized. Results Acute gastrointestinal symptoms occurred in 7 cases and fever in 5 cases. Renal insufficiency and maintenance hemodialysis in 3 cases, 8 cases of hypertension, 6 cases of surgical history. In clinical diagnosis, 5 cases of intestinal obstruction, 6 cases of severe infection and septic shock. Only 3 of the 10 patients survived. Both patients treated with surgery were diagnosed with intestinal necrosis. The gas in portal vein was mainly distributed in the left branch of portal vein. There were 7 cases of pneumatosis of splenic vein, superior mesenteric vein and its tributaries, and 9 cases of pneumatosis of intestinal wall. There were 7 cases of local intestinal wall edema, 5 cases of intestinal obstruction and 3 cases of digestive tract perforation. Enhanced scan confirmed superior mesenteric artery thrombosis in 2 cases. Conclusion The incidence of pneumatosis cystoides intestinalis in HPVG cases is high. Clinical attention should be paid to the identification of HPVG and related imaging features, so as to intervene in patients in time. -

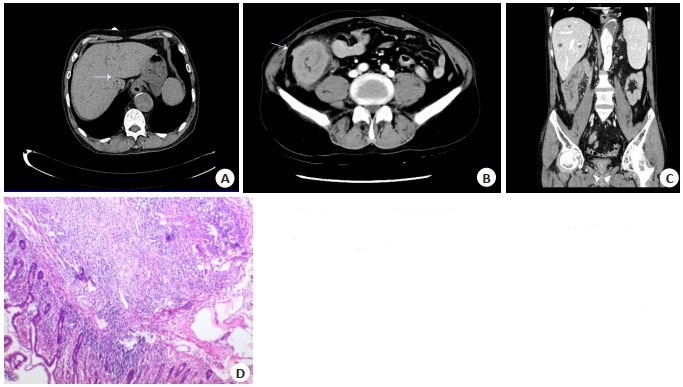
图 1 病例7的CT及病理切片图
Figure 1. CT image and pathological section of case 7
A-C: CT image on the day of admission. A: HPVG was mainly distributed in the distal left branch of the portal vein; B: Multiple small vesicles, strip-like gas accumulation (white arrow) under the intestinal wall; C: The distal part of superior mesenteric vein belongs to the branch with accumulated gas (white arrow). D-E: CT images reviewed. D: A large amount of free gas in the abdominal cavity (white arrow); E: The intestinal wall of the transverse colon near the splenic flexure is edematous, with exudation around it (white arrow); F: Transverse colon pathological section (HE staining, ×100), lesion area intestinal mucosal erosion with inflammatory exudative necrosis, inflammatory cell infiltration, and histiocytes aggregation.

图 2 病例1的CT及病理切片图
Figure 2. CT image and pathological section of case 1
A: A small amount of short linear gas shadow (white arrow) under the capsule of the left lobe and caudate lobe of the liver; B, C: CT reexamination of the next day showed that the wall of ascending colon had obvious thickening and uneven enhancement, and exudation and small lymph nodes were seen around it; D: Pathological section of ascending colon (HE staining, × 400), mucosal erosion, bleeding, submucosal edema, and small vessel hyperplasia.

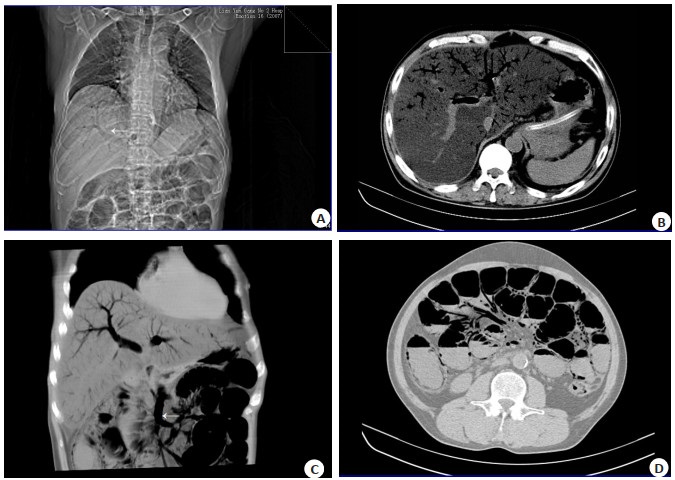
图 3 病例4的CT表现
Figure 3. CT image of case 4
A: The localization image showed a "withered branch" gas shadow (white arrow) in the liver, and the intestinal tract was inflated and dilated; B: A large amount of gas shadows could be seen in the left and right branches and main trunk of the portal vein, with the left branch being the main one; C: Coronary MIP reconstruction showed that the portal vein had obvious air accumulation and appeared as a "withered branch", and the superior mesenteric vein and its branches had obvious air accumulation (white arrow); D: The intestines were inflated and dilated, with multiple flat air and liquid, multiple vesicular gas shadows under the intestinal wall (white arrow), and obvious gas accumulation in the branches of superior mesenteric vein (white arrow).
表 1 10例HPVG患者临床资料
Table 1. Clinical data of 10 patients with HPVG
Case Gender/Age (years) Medical history Underlying disease Main diagnosis Main treatments Prognosis 1 Male/59 Abdominal pain with diarrhea and vomiting after eating Chronic renal insufficiency, postrenal transplantation, maintenance hemodialysis; postoperative aortic coarctation (Standford type B), hypertension; post-operative spinal fracture Ischemic intestinal necrosis Surgical operations Survival 2 Male/87 Diarrhea for 4 d, abdominal pain for more than 1 d, with vomiting Hypertension Ischemic intestinal necrosis Symptomatic support Survival 3 Male/79 1 week after total gastrectomy, vomiting, abdominal pain, and fever for 1 d Hypertension Duodenal stump fistula and abdominal infection after total gastrectomy for cardiac cancer Symptomatic support Survival 4 Male/52 Vomiting (vomiting blood) with confusion after alcohol abuse Alcoholism, high blood pressure Upper gastrointestinal bleeding with hemorrhagic shock, multiple organ failure Symptomatic support Death 5 Male/63 Abdominal pain with nausea for 12 h Chronic renal insufficiency, maintenance hemodialysis; hypertension, gout, rheumatoid arthritis; postoperative right femoral neck fracture Severe infection with septic shock, gastrointestinal perforation Symptomatic support, refused surgery Death 6 Male/76 Fatigue, anorexia for more than 5 years, fever for 12 d, accompanied by diarrhea and vomiting. Chronic renal insufficiency, maintenance hemodialysis; hypertension, diabetes, cerebral infarction; postcholecystectomy Severe infection with septic shock, upper gastrointestinal bleeding, metabolic acidosis Symptomatic support Death 7 Male/48 Fever for 2 d, chest tightness for 1 d Hypertension, asthma, postoperative right knee fracture Severe myocarditis with cardiogenic shock, severe pneumonia with ARDS (moderate), sepsis, septic shock Surgical operations Death 8 Female/30 Postpartum hemorrhage, hysterectomy, 3 d after cardiopulmonary resuscitation No Postpartum massive bleeding, after hysterectomy; Ischemic hypoxic encephalopathy after cardiopulmonary resuscitation surgery; Abdominal infection and septic shock; Multiple organ failure; DIC Symptomatic support Death 9 Male/88 After severe craniocerebral trauma, disturbance of consciousness for 10 d, fever for 8 d. Cardiac dysfunction, paroxysmal atrial fibrillation; postoperative inguinal hernia Severe craniocerebral trauma, pulmonary infection, respiratory failure, septic shock Symptomatic support Death 10 Male/43 Abdominal pain and fever for 3 d, diarrhea and vomiting for 1 d. Hypertension Abdominal infection, septic shock Symptomatic support Death HPVG: Hepatic portal vein gas.  下载: 导出CSV
下载: 导出CSV
表 2 10例HPVG患者影像学特征
Table 2. Imaging features of 10 patients with HPVG
Case Distribution of HPVG Gas accumulation in SMV and splenic vein PCI SMA thrombosis Edema of intestinal wall Intestinal obstruction Gastrointestinal perforation 1 A small amount in left branch distal and caudate lobe No No Yes Yes No No 2 A small amount in left branch distal Yes Yes Yes Yes No No 3 A small amount in left branch distal No Yes No enhanced scan No No No 4 A large amount in left and right branch, the left branch is obvious Yes Yes No enhanced scan None Yes No 5 A small amount in left branch distal Yes Yes No Yes No Yes 6 Left branch distal Yes Yes No Yes Yes No 7 Left branch, a small amount in distal right branch Yes Yes No Yes Yes Yes 8 A small amount in left branch distal No Yes No enhanced scan Yes Yes No 9 A large amount in left and right branch Yes Yes No enhanced scan No No Yes 10 Left branch distal Yes Yes No enhanced scan Yes Yes No SMA: Superior mesenteric artery; SMV: Superior mesenteric vein; PCI: Pneumatosis cystoides intestinalis.
下载: 导出CSV
-
[1] Abboud B, Hachem JE, Yazbeck T, et al. Hepatic portal venous gas: Physiopathology, etiology, prognosis and treatment[J]. World J Gastroenterol, 2009, 15(29): 3585. doi: 10.3748/wjg.15.3585 [2] Seak CJ, Yen DHT, Ng CJ, et al. Rapid Emergency Medicine Score: a novel prognostic tool for predicting the outcomes of adult patients with hepatic portal venous gas in the emergency department[J]. PLoS One, 2017, 12(9): e0184813. doi: 10.1371/journal.pone.0184813 [3] Koizumi C, Michihata N, Matsui H, et al. In-hospital mortality for hepatic portal venous gas: analysis of 1590 patients using a Japanese national inpatient database[J]. World J Surg, 2018, 42(3): 816- 22. doi: 10.1007/s00268-017-4189-y [4] Chen HM, Wu QS, Fang HC, et al. Intestinal necrosis cannot be neglected in a patient with hepatic portal vein gas combined with appendicitis: a rare case report and literature review[J]. BMC Surg, 2019, 19(1): 1-6. doi: 10.1186/s12893-018-0463-7 [5] 刘扑琼, 汤敏, 张长顺. CT诊断肝门静脉积气2例报告[J]. 中国临床医学, 2015, 22(3): 425-6. https://www.cnki.com.cn/Article/CJFDTOTAL-LCYX201503045.htm [6] 张莹, 刘欣, 张文耀, 等. 螺旋CT检查急性缺血性肠病所致门静脉和肠壁积气的表现特点及其临床诊断价值研究[J]. 实用肝脏病杂志, 2018, 21(5): 793-6. https://www.cnki.com.cn/Article/CJFDTOTAL-GBSY201805035.htm [7] 魏明华. 门静脉积气CT表现2例[J]. 中国中西医结合影像学杂志, 2017, 15(3): 376-7. https://www.cnki.com.cn/Article/CJFDTOTAL-JHYX201703042.htm [8] 曹利军, 杨翔, 黎命娟, 等. 肝门静脉积气四例临床分析[J]. 中华普通外科杂志, 2019, 34(8): 725-6. [9] 朱志韬, 孙志先, 祖茂衡. 门静脉、肠系膜静脉积气死亡1例[J]. 肝脏, 2016, 21(9): 800. https://www.cnki.com.cn/Article/CJFDTOTAL-ZUAN201609029.htm [10] Wolfe J, Evans WA. Gas in the portal veins of the liver in infants; a roentgenographic demonstration with postmortem anatomical correlation[J]. Am J Roentgenol Radium Ther Nucl Med, 1955, 74 (3): 486-8. [11] Susman N, Senturia HR. Gas embolization of the portal venous system[J]. Am J Roentgenol Radium Ther Nucl Med, 1960, 83: 847-50. [12] Dashwood AM, Mason R, Jennings C, et al. Hepatic portal venous gas with associated bowel ischaemia and intra-abdominal sepsis after recent chemotherapy[J]. BMJ Case Rep, 2016: bcr2015213564. doi: 10.1136/bcr-2015-213564 [13] Li ZM, Su YZ, Wang XJ, et al. Hepatic portal venous gas associated with colon cancer[J]. Medicine, 2017, 96(50): e9352. doi: 10.1097/MD.0000000000009352 [14] Capolupo GT, Mascianà G, Carannante F, et al. Hepatic portal venous gas after colonoscopy: a case report and review[J]. Int J Surg Case Rep, 2018, 51: 54-7. doi: 10.1016/j.ijscr.2018.06.041 [15] Ikegame K, Iimuro Y, Furuya K, et al. A case with hepatic portal vein gas who required delayed elective surgery[J]. Int J Surg Case Rep, 2019, 65: 233-7. doi: 10.1016/j.ijscr.2019.10.085 [16] Oei T, VanSonnenberg E, Shankar S, et al. Radiofrequency ablation of liver tumors: a new cause of benign portal venous gas[J]. Radiology, 2005, 237(2): 709-17. doi: 10.1148/radiol.2372041295 [17] Liu C, Wu CH, Zheng XD, et al. Hepatic portal venous gas: a case report and analysis of 131 patients using PUBMED and MEDLINE database[J]. Am J Emerg Med, 2021, 45: 506-9. doi: 10.1016/j.ajem.2020.06.085 [18] Gosink BB. Intrahepatic gas: differential diagnosis[J]. Am J Roentgenol, 1981, 137(4): 763-7. doi: 10.2214/ajr.137.4.763 [19] Sugihara Y, Okada H. Pneumatosis cystoides intestinalis[J]. N Engl J Med, 2017, 377(23): 2266. [20] Pear BL. Pneumatosis intestinalis: a review[J]. Radiology, 1998, 207(1): 13-9. [21] Mazzei M A, Guerrini S, Cioffi SN, et al. Diagnosis of acute mesenteric ischemia/infarction in the era of multislice CT[J]. Recenti Prog Med, 2012, 103(11): 435-7. [22] Khalil PN, Huber-Wagner S, Ladurner R, et al. Natural history, clinical pattern, and surgical considerations of pneumatosis intestinalis[J]. Eur J Med Res, 2009, 14(6): 231-9. [23] Keyting WS, McCarver RR, Kovarik JL, et al. Pneumatosis intestinalis: a new concept[J]. Radiology, 1961, 76(5): 733-41. [24] Florim S, Almeida A, Rocha D, et al. Acute mesenteric ischaemia: a pictorial review[J]. Insights Imaging, 2018, 9(5): 673-82. [25] Hussain A, Mahmood H, El-Hasani S. Portal vein gas in emergency surgery[J]. World J Emerg Surg, 2008, 3: 21. [26] Kinoshita H. Clinical features and management of hepatic portal venous gas[J]. Arch Surg, 2001, 136(12): 1410. [27] Fitzpatrick LA, Rivers-Bowerman MD, Thipphavong S, et al. Pearls, pitfalls, and conditions that mimic mesenteric ischemia at CT[J]. RadioGraphics, 2020, 40(2): 545-61. [28] Feczko PJ, Mezwa DG, Farah MC, et al. Clinical significance of pneumatosis of the bowel wall[J]. RadioGraphics, 1992, 12(6): 1069-78. [29] Liebman PR, Patten MT, Manny J, et al. Hepatic: portal venous gas in adults: etiology, pathophysiology and clinical significance[J]. Ann Surg, 1978, 187(3): 281-7. [30] Bloom RA, Lebensart PD, Levy P, et al. Survival after ultrasonographic demonstration of portal venous gas due to mesenteric artery occlusion[J]. Postgrad Med J, 1990, 66(772): 137-9. [31] Lassandro G, Picchi SG, Romano F, et al. Intestinal pneumatosis: differential diagnosis[J]. Abdom Radiol, 2022, 47(5): 1529-40. [32] Kunishi Y, Ota M, Kato Y, et al. Pneumatosis cystoides intestinalis: lung window setting on CT[J]. Clin Case Rep, 2017, 5(11): 1896-7. -

 点击查看大图
点击查看大图

计量
- 文章访问数: 143
- HTML全文浏览量: 122
- PDF下载量: 12
- 被引次数: 0