



Value of CT in the differential diagnosis of lung invasive adenocarcinoma and minimally invasive adenocarcinoma
-
摘要:
目的 探究CT鉴别肺浸润性腺癌(IAC)与肺微浸润性腺癌(MIA)的价值。 方法 选取2020年1月~2021年12月在我院接受手术治疗的肺磨玻璃结节患者共120例作为研究对象。将经活检穿刺或术后病理诊断为IAC的75例患者作为IAC组,45例MIA患者作为MIA组。对比两组CT影像学资料,采用ROC曲线评估CT鉴别IAC与MIA价值。 结果 IAC组与MIA组结节部位、边缘清晰/模糊、胸膜凹陷征及病灶CT密度值的差异无统计学意义(P>0.05);IAC组结节最大直径及最大密度区域CT值高于MIA组(P < 0.05),且IAC组结节形态不规则、分叶征、毛刺征、血管集束征占比高于MIA组(P < 0.05)。Logistic多因素回归分析结果显示,结节最大直径、分叶征、毛刺征、血管集束征、最大密度区域CT值是导致病理结果性质出现差异的相关危险因素(P < 0.05)。ROC曲线显示,结节最大直径约登指数(0.636)最大时对应截断值为1.31 cm,曲线下面积(AUC)为0.846,鉴别IAC与MIA的敏感度、特异性分别为75.56%、88.00%;分叶征鉴别IAC与MIA的AUC为0.713,敏感度、特异性分别为66.67%、76.00%;毛刺征鉴别IAC与MIA的AUC为0.731,敏感度、特异性分别为68.89%、77.33%;血管集束征鉴别IAC与MIA的AUC为0.744,敏感度、特异性分别为75.56%、73.33%;最大密度区域CT值约登指数(0.542)最大时对应截断值为-531.75 Hu,鉴别IAC与MIA的AUC为0.801,敏感度、特异性分别为68.89%、85.33%。 结论 CT技术在鉴别IAC与MIA中具有较高的指导作用,结节直径、最大密度区域CT值、分叶征、毛刺征、血管集束征对于IAC与MIA的临床鉴别具有重要价值。 Abstract:Objective To explore the value of CT in the differential diagnosis of lung invasive adenocarcinoma (IAC) and minimally invasive adenocarcinoma (MIA). Methods A total of 120 patients with lung ground glass nodules who underwent surgical treatment in our hospital from January 2020 to December 2021 were selected. Among the patients, 75 cases with IAC diagnosed by biopsy or postoperative pathology were enrolled as IAC group, and 45 cases with MIA were included in MIA group. The CT imaging data of the two groups were compared, and ROC curve was used to evaluate the value of CT in differentiating IAC from MIA. Results There were no statistical differences in nodule location, clear/fuzzy edge, pleural indentation sign and lesion CT density between IAC group and MIA group (P>0.05). However, the maximum nodule diameter and CT value at the maximum density area in IAC group were higher than those in MIA group (P < 0.05), and the proportions of irregular nodule morphology, lobulation sign, spiculation sign and vascular convergence sign were also higher in IAC group than those in MIA group (P < 0.05). The maximum nodule diameter, lobulation sign, spiculation sign, vascular convergence sign and CT value at the maximum density area were the related risk factors leading to the differences in pathological results (P < 0.05). ROC results showed that when the Youden index of the maximum nodule diameter was the maximum (0.636), the corresponding cut-off value, AUC, sensitivity and specificity in differentiating IAC from MIA were 1.31 cm, 0.846, 75.56% and 88.00%, respectively. The AUC, sensitivity and specificity in differentiating IAC from MIA were 0.713, 66.67% and 76.00% of lobulation sign, were 0.731, 68.89% and 77.33% of spiculation sign, and were 0.744, 75.56% and 73.33% of vascular convergence sign respectively. When the Youden index of CT value at the maximum density area was the maximum at 0.542, the corresponding cut-off value was -531.75 Hu, and the AUC, sensitivity and specificity in the differential diagnosis of IAC and MIA were 0.801, 68.89% and 85.33%, respectively. Conclusion CT technology has a high guiding role in the differential diagnosis of IAC and MIA. Nodule diameter, CT value at the maximum density area, lobulation sign, spiculation sign and vascular convergence sign are of great value for the clinical differentiation of IAC and MIA. -

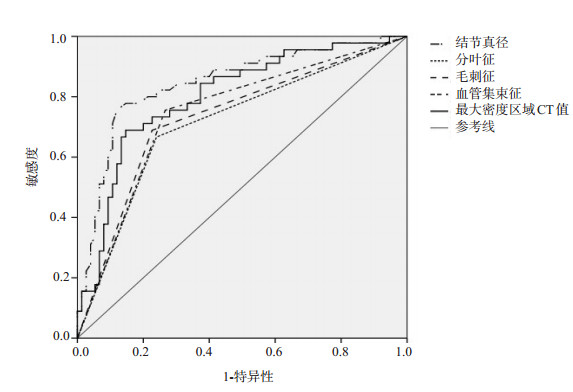
图 1 CT征象特点鉴别IAC与MIA的ROC曲线
Figure 1. ROC curves of CT signs in differentiating IAC from MIA.

图 2 典型病例CT扫描图像
患者男, 47岁. A~B: CT下可见右肺上叶磨玻璃结节, 形态膨胀, 无毛刺、分叶, 其内血管穿行明显增粗; C~D: CT下可见左肺下叶磨玻璃结节, 浅分叶、血管集束征、胸膜牵拉.
Figure 2. CT scan images of typical cases.
表 1 IAC组与MIA组CT征象特点比较
Table 1. Comparison of CT signs between IAC group and MIA group [n(%)]
CT征象 IAC组(n=75) MIA组(n=45) χ2/t P 结节最大直径(cm, Mean±SD) 1.59±0.45 1.01±0.31 7.623 < 0.001 部位 0.010 0.919 左肺 24(32.00) 14(31.11) 右肺 51(68.00) 31(68.89) 形态 5.433 0.020 规则 18(24.00) 20(44.44) 不规则 57(76.00) 25(55.56) 边缘 清晰 56(74.67) 33(73.33) 0.026 0.872 模糊 19(25.33) 12(26.67) 分叶征 52(69.33) 21(46.67) 6.065 0.014 毛刺征 53(70.67) 19(42.22) 9.481 0.002 血管集束征 13.657 < 0.001 有 51(68.00) 15(33.33) 无 24(32.00) 30(66.67) 胸膜凹陷征 0.960 0.327 有 21(28.00) 9(20.00) 无 54(72.00) 36(80.00) 最大密度区域CT值(Hu, Mean±SD) -422.69±131.45 -554.45±122.37 5.553 < 0.001 IAC: 浸润性腺癌; MIA: 微浸润性腺癌.  下载: 导出CSV
下载: 导出CSV
表 2 GGNs结节CT表现对病理性质的影响
Table 2. Effects of CT findings of GGNs nodules on pathological properties
因素 β SE Wald χ2 OR 95% CI P 结节最大直径 1.562 0.596 6.869 4.768 1.483~15.335 0.009 形态 0.936 0.13 46.678 2.550 1.949~3.335 2.934 分叶征 1.365 0.386 12.505 3.916 1.838~8.344 < 0.001 毛刺征 1.578 0.576 7.505 4.845 1.567~14.984 0.006 血管集束征 0.165 0.051 10.467 1.179 1.067~1.303 0.001 最大密度区域CT值 0.820 0.369 4.938 2.270 1.102~4.680 0.027
下载: 导出CSV
表 3 CT征象特点鉴别IAC与MIA的价值
Table 3. Value of CT signs in differentiating IAC from MIA
指标 Cut-off AUC 敏感性(%) 特异性(%) 约登指数 95%CI 结节最大直径 ≥1.31 cm 0.846 75.56 88.00 0.636 0.770~0.922 分叶征 - 0.713 66.67 76.00 0.427 0.628~0.798 毛刺征 - 0.731 68.89 77.33 0.462 0.648~0.814 血管集束征 - 0.744 75.56 73.33 0.489 0.663~0.825 最大密度区域CT值 ≥-531.75 Hu 0.801 68.89 85.33 0.542 0.718~0.868
下载: 导出CSV
-
[1] 蔡俊辉, 段绍峰, 袁虎, 等. 机器学习鉴别表现为肺纯磨玻璃结节的浸润性腺癌与非浸润性腺癌[J]. 中国医学影像技术, 2020, 36(3): 405-10. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYXX202003026.htm [2] 金志发, 陈相猛, 冯宝, 等. CT纹理特征分析鉴别诊断表现为肺部亚实性结节的微浸润腺癌和浸润性腺癌[J]. 中国医学影像技术, 2019, 35(5): 691-5. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYXX201905017.htm [3] 叶钉利, 姜雯, 吴佳妮, 等. 基于CT影像组学模型预测肺原位腺癌及微浸润腺癌与浸润性腺癌[J]. 中国医学影像技术, 2020, 36(9): 1345-9. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYXX202009019.htm [4] 朱红霞, 张光辉, 林平. CT影像磨玻璃样结节中实性成分对肺腺癌的诊断价值分析[J]. 中国基层医药, 2020, 27(9): 1128-30. https://www.cnki.com.cn/Article/CJFDTOTAL-YXYY201712056.htm [5] 虞梁, 王俊, 李洪, 等. 肺磨玻璃结节CT影像征象鉴别诊断肺浸润性腺癌与微浸润腺癌[J]. 南京医科大学学报: 自然科学版, 2020, 40(2): 248-51. https://www.cnki.com.cn/Article/CJFDTOTAL-NJYK202002019.htm [6] 游杰, 张国中, 高祥龙, 等. PET/CT联合CT三维重建在鉴别早期肺腺癌不同病理亚型中的价值[J]. 中国肺癌杂志, 2021, 24(7): 468-74. https://www.cnki.com.cn/Article/CJFDTOTAL-FAIZ202107003.htm [7] 汪升蛟, 宋正波, 吕镗烽. 术后IB期浸润性肺腺癌不同病理亚型的预后分析[J]. 东南国防医药, 2019, 21(3): 234-9. https://www.cnki.com.cn/Article/CJFDTOTAL-DNGY201903003.htm [8] 王敏可, 杨海, 张敏鸽, 等. 肺浸润性腺癌不同病理分类的临床及CT特征比较[J]. 浙江医学, 2021, 43(12): 1337-40. https://www.cnki.com.cn/Article/CJFDTOTAL-ZJYE202112029.htm [9] 黄超, 王涛, 邱志新, 等. 不同病理类型肺腺癌临床和影像特征及预后分析[J]. 现代肿瘤医学, 2022, 30(14): 2548-53. https://www.cnki.com.cn/Article/CJFDTOTAL-SXZL202214013.htm [10] 吕燕, 叶靖, 凌俊. 纹理分析评估肺磨玻璃结节样腺癌的浸润性: 基于CT平扫与增强图像的对照研究[J]. 放射学实践, 2021, 36(12): 1503-8. https://www.cnki.com.cn/Article/CJFDTOTAL-FSXS202112009.htm [11] 秦福兵, 陆友金. 纯磨玻璃结节定量CT鉴别肺浸润性腺癌与浸润前病变和微浸润腺癌[J]. 中国医学计算机成像杂志, 2016, 22(1): 22-6. https://www.cnki.com.cn/Article/CJFDTOTAL-YJTY201601007.htm [12] Junji, Ichinose, Utility of maximum CT value in predicting the invasiveness of pure ground-glass nodules[J]. Clin Lung Cancer, 2020, 21(3): 281-7. [13] 李敏, 王娅菲, 姜文蓁, 等. 双层探测器光谱CT平扫定性联合定量参数预测肺纯磨玻璃结节侵袭性的价值[J]. 中华放射学杂志, 2022, 56(3): 248-53. [14] 左玉强, 冯平勇, 孟庆春, 等. 肺纯磨玻璃结节微浸润腺癌与浸润性腺癌的CT鉴别诊断[J]. 临床放射学杂志, 2017, 36(4): 495-8. https://www.cnki.com.cn/Article/CJFDTOTAL-LCFS201704013.htm [15] Lu J, Tang HT, Yang XG, et al. Diagnostic value and imaging features of multi-detector CT in lung adenocarcinoma with ground glass nodule patients[J]. Oncol Lett, 2020, 20(1): 693-8. [16] 胡建华, 曾春意, 张为, 等. 肺微浸润性腺癌和浸润性腺癌的CT定量参数及影像学特征鉴别诊断价值[J]. 分子影像学杂志, 2022, 45(2): 204-9. doi: 10.12122/j.issn.1674-4500.2022.02.08 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 399
- HTML全文浏览量: 109
- PDF下载量: 12
- 被引次数: 0