



Comparation of CT enterography imaging features between colonic Crohn's disease and ulcerative colitis with clinical
-
摘要:
目的 探究CT小肠造影(CTE)对结肠型克罗恩病与溃疡性结肠炎的诊断及鉴别诊断价值。 方法 选取蚌埠医学院第一附属医院和南京中医药大学附属江苏省中医院于2019年1月~2022年1月收治的结肠型克罗恩病患者36例和溃疡性结肠炎患者36例行CTE检查,分别观察两组影像特征,结合实验室指标、临床表现对克罗恩病和溃疡性结肠炎患者进行回顾性分析。 结果 36例克罗恩病患者中,CTE影像示肠壁不均匀增厚21例、肠道狭窄22例、瘘管形成7例及累及升结肠21例,均高于溃疡性结肠炎患者,差异有统计学意义(P < 0.05);36例溃疡性结肠炎患者,粘液便18例及血便22例高于克罗恩病患者(P < 0.05),溃疡性结肠炎患者平均发病年龄较结肠型克罗恩病患者平均发病年龄大(P < 0.05)。克罗恩病患者与溃疡性结肠炎患者的C反应蛋白及红细胞沉降率含量均值分别为28.17 mg/L vs 17.67 mg/L、32.25 mm/h vs 22.95 mm/h;C反应蛋白及红细胞沉降率含量的平均值对克罗恩病与溃疡性结肠炎的鉴别无统计学意义(P > 0.05)。 结论 通过CTE影像特征更直观地对结肠型克罗恩病与溃疡性结肠炎进行鉴别,结合临床、内镜表现及病理诊断,为治疗方案设计提供更可靠的依据。 Abstract:Objective To investigate the diagnostic and differential diagnostic value of CT enterography for colon-type Crohn's disease and ulcerative colitis. Methods Thirty-six patients with colonic Crohn's disease and 36 patients with ulcerative colitis admitted to the First Affiliated Hospital of Bengbu Medical College and Jiangsu Provincial Hospital of Nanjing University of Traditional Chinese Medicine from January 2019 to January 2022 were selected for CT enterography examination. The imaging features of both were observed. The patients with Crohn's disease and ulcerative colitis were retrospectively analyzed by combining laboratory indices and clinical manifestations. Results Among the 36 patients with Crohn's disease, CT enterography images showed 21 cases of uneven thickening of the intestinal wall, 22 cases of intestinal stricture, 7 cases of fistula formation, and 21 cases of involvement of the ascending colon were higher than those of patients with ulcerative colitis (P < 0.05). Among the 36 patients with ulcerative colitis, 18 cases of mucus stools and 22 cases of bloody stools were higher than those of patients with Crohn's disease (P < 0.05). The mean age of onset was older in patients with ulcerative colitis than in patients with colonic Crohn's disease(P < 0.05). The mean values of C-reactive protein and erythrocyte sedimentation rate in patients with Crohn's disease were 28.17 mg/L and 32.25 mm/h, respectively. The mean values of C-reactive protein and erythrocyte sedimentation rate in patients with ulcerative colitis were 17.67 mg/L and 22.95 mm/h, respectively. The mean values of C-reactive protein and erythrocyte sedimentation rate were not statistically significant for the differentiation of Crohn's disease from ulcerative colitis (P > 0.05). Conclusion The CT enterography imaging features can be used to differentiate colon-type Crohn's disease from ulcerative colitis more visually. It provides a more reliable basis for treatment plan design by combining clinical, endoscopic manifestations and pathological diagnosis. -
Key words:
- colonic Crohn's disease /
- ulcerative colitis /
- CT enterography /
- differential diagnosis
-

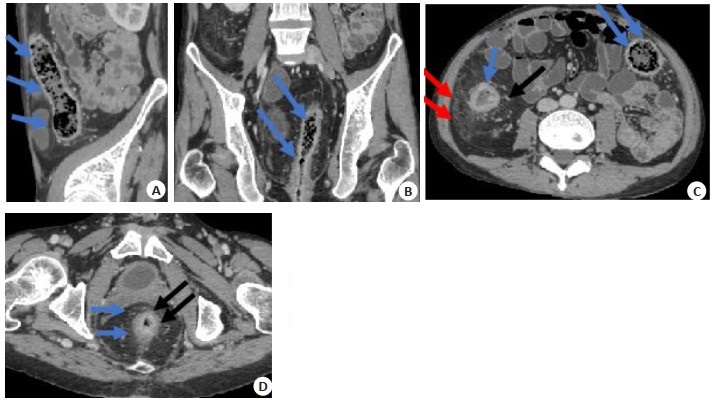
图 1 某结肠型CD患者CTE影像表现
男性CD患者, 50岁, 腹泻伴肛内分泌物流出, 无明显腹痛, 近期体质量变化不大. A~B: CT增强轴位及矢状位示直肠肠壁增厚(蓝色箭头), 伴肛周脓肿形成(红色箭头); C~E: CT平扫+增强冠状位及轴位示乙状结肠肠壁肠壁不均匀增厚伴强化(蓝色箭头).
Figure 1. Imaging findings of CTE in a patient with colorectal CD.

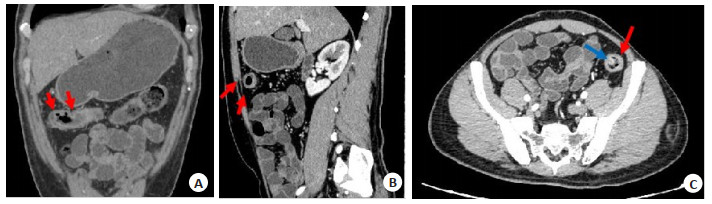
图 2 某结肠型CD患者CTE影像表现
男性CD患者, 26岁, 腹痛腹泻, 粘液脓血便, 近期体质量减轻, 确诊为全结肠CD. CT横断面增强示直肠、乙状结肠、升结肠及降结肠管壁增厚, 部分呈分层强化(黑色箭头所示), 升结肠周围炎性渗出(红色箭头).
Figure 2. Imaging findings of CTE in a patient with colonic CD.

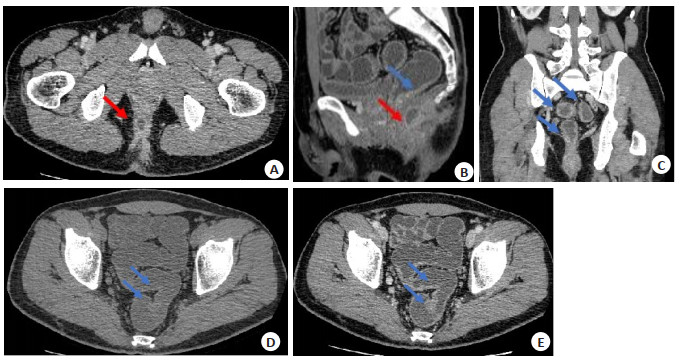
图 3 某UC患者CTE影像表现
男性UC患者, 43岁, 腹痛腹泻、稀水样便伴脓血, 病程中患有口腔溃疡, CT冠、矢、轴状位增强示降结肠及横结肠肝曲管壁增厚伴强化, 呈对称性改变, 周围脂肪间隙清晰(如红色箭头所示). CTE轴状位显示降结肠内增强的黏膜结节(蓝色箭头所示), 与结肠镜显示降结肠息肉相符.
Figure 3. Imaging manifestations of CTE in UC patients.
表 1 CD及UC的临床资料比较
Table 1. Comparison of clinical data of CD group and UC group (n=36)
项目 CD组 UC组 χ2/t/Z P 性别[n(%)] 1.000 0.317 男 22(61.1) 26(72.2) 女 14(38.9) 10(27.8) 发病年龄(岁, Mean±SD) 32.89±16.78 43.19±13.72 -2.851 0.006 腹痛[n(%)] 28(77.8) 29(80.6) 0.084 0.772 腹泻[n(%)] 27(75.0) 26(72.2) 0.071 0.789 呕吐[n(%)] 2(5.6) 0(0) - 0.493* 消瘦[n(%)] 15(41.7) 10(27.8) 1.532 0.216 粘液便[n(%)] 5(13.9) 18(50) 10.797 0.001 便秘[n(%)] 3(8.3) 2(5.6) - 1.000* 血便[n(%)] 13(36.1) 22(61.1) 4.503 0.034 发热[n(%)] 3(8.3) 2(5.6) - 1.000* 肛瘘[n(%)] 5(13.9) 0(0) - 0.020* 肛周脓肿[n(%)] 13(36.1) 0(0) - < 0.001* CRP[mg/L, M(P25, P75)] 28.17(7.90, 34.97) 17.67(1.70, 22.36) -1.960 0.050 ESR [mm/h, M(P25, P75)] 32.25(11.50, 38.75) 22.95(8.25, 34.60) -1.025 0.305 st-OB[n(%)] 13(36.1) 22(77.0) 4.503 0.034 *采用Fisher精确检验. UC: 溃疡性结肠炎; CD: 克罗恩病; CRP: C反应蛋白; ESR: 红细胞沉降率; st-OB: 隐血实验.  下载: 导出CSV
下载: 导出CSV
表 2 CD及UC的CTE影像特征比较
Table 2. Comparison of CTE imaging features between CD and UC [n(%)]
CTE征象 CD组 UC组 χ2/Fisher P 肠壁增厚 6.854 0.009 环周均匀增厚 15(41.7) 26(72.7) 不对称性增厚 21(58.3) 10(27.8) 肠壁强化 1.481 0.224 分层强化 16(44.4) 11(30.6) 非分层强化 20(55.6) 25(69.4) 肠道不规则狭窄 22(61.1) 12(33.3) 5.573 0.018 梳征 21(58.3) 15(41.7) 2.000 0.157 周围脂肪间隙增宽 23(63.9) 14(38.9) 4.503 0.034 周围炎性渗出 24(66.7) 7(19.4) 16.371 < 0.001 肠周淋巴结增生 19(52.8) 17(47.2) 0.222 0.637 瘘管 7(19.4) 0(0) - 0.011* CTE: CT小肠造影; *采用Fisher精确检验.
下载: 导出CSV
表 3 CD与UC发病部位的比较
Table 3. Comparison of sites of CD and UC (n)
部位 CD UC χ2 P 直肠 18 25 2.829 0.093 乙状结肠 21 29 4.189 0.041 降结肠 33 27 3.600 0.058 横结肠 27 25 0.277 0.599 升结肠 21 10 6.854 0.009 盲肠 9 7 0.321 0.571
下载: 导出CSV
-
[1] Ng SC, Shi HY, Hanmidi N, et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies[J]. Lancet, 2017, 390(10114): 2769-78. doi: 10.1016/S0140-6736(17)32448-0 [2] Kaplan GG. The global burden of IBD: from 2015 to 2025[J]. Nat Rev Gastroenterol Hepatol, 2015, 12(12): 720-7. doi: 10.1038/nrgastro.2015.150 [3] Wright EK, Ding NS, Niewiadomski O. Management of inflammatory bowel disease[J]. Med J Aust, 2018, 209(7): 318-23. doi: 10.5694/mja17.01001 [4] Guan QD. A comprehensive review and update on the pathogenesis of inflammatory bowel disease[J]. J Immunol Res, 2019, 2019: 7247238. [5] Satsangi J, Silverberg MS, Vermeire S, et al. The Montreal classification of inflammatory bowel disease: controversies, consensus, and implications[J]. Gut, 2006, 55(6): 749-53. doi: 10.1136/gut.2005.082909 [6] Flynn S, Eisenstein S. Inflammatory bowel disease presentation and diagnosis[J]. Surg Clin North Am, 2019, 99(6): 1051-62. doi: 10.1016/j.suc.2019.08.001 [7] Tontini GE, Vecchi M, Pastorelli L, et al. Differential diagnosis in inflammatory bowel disease colitis: state of the art and future perspectives[J]. World J Gastroenterol, 2015, 21(1): 21-46. doi: 10.3748/wjg.v21.i1.21 [8] 周杰, 李彪, 孔德灿, 等. 结肠型克罗恩病与溃疡性结肠炎的临床影像特征对比分析[J]. 中华炎性肠病杂志, 2021, 5(4): 308-13. doi: 10.3760/cma.j.cn101480-20210610-00045 [9] Ma L, Shen X, Chen YJ, et al. Computed tomography enterography for crohn's disease: correlation between the imaging findings and histopathologic scoring system[J]. Abdom Radiol, 2021, 46(9): 4121-9. doi: 10.1007/s00261-021-03112-w [10] Jia YM, Li C, Yang XY, et al. CT Enterography score: a potential predictor for severity assessment of active ulcerative colitis[J]. BMC Gastroenterol, 2018, 18(1): 173. doi: 10.1186/s12876-018-0890-z [11] 陆瑜, 蔡瑾, 张蓓, 等. 克罗恩病小肠CT造影活动度分级与粪便乳铁蛋白相关性的研究[J]. 临床放射学杂志, 2022, 41(3): 509-13. https://www.cnki.com.cn/Article/CJFDTOTAL-LCFS202203022.htm [12] Zhang YZ, Li YY. Inflammatory bowel disease: pathogenesis[J]. World J Gastroenterol, 2014, 20(1): 91-9. doi: 10.3748/wjg.v20.i1.91 [13] Malik TA. Inflammatory bowel disease: historical perspective, epidemiology, and risk factors[J]. Surg Clin North Am, 2015, 95(6): 1105-22, v. doi: 10.1016/j.suc.2015.07.006 [14] 辛丽敏, 李楠. C反应蛋白在炎症性肠病中的应用及价值[J]. 胃肠病学和肝病学杂志, 2013, 22(6): 600-3. [15] 赵甲秀. 溃疡性结肠炎与结肠克罗恩病病理诊断的鉴别分析[J]. 中国现代药物应用, 2020, 14(1): 46-8. https://www.cnki.com.cn/Article/CJFDTOTAL-ZWYY202001024.htm [16] 周敏清, 谢宝君. 克罗恩病的小肠CTE联合CTA诊断[J]. 放射学实践, 2015, 30(4): 364-8. https://www.cnki.com.cn/Article/CJFDTOTAL-FSXS201504023.htm [17] 中华医学会消化病学分会炎症性肠病学组. 炎症性肠病诊断与治疗的共识意见(2012年, 广州)[J]. 中华消化杂志, 2012(12): 796-813. doi: 10.3760/cma.j.issn.0254-1432.2012.12.002 [18] 吴开春, 梁洁, 冉志华, 等. 炎症性肠病诊断与治疗的共识意见(2018年·北京)[J]. 中国实用内科杂志, 2018, 38(9): 796-813. https://www.cnki.com.cn/Article/CJFDTOTAL-SYNK201809007.htm [19] Smith P, Bénézech C. Creeping fat in crohn's disease: innocuous or innocuum?[J]. Immunity, 2020, 53(5): 905-7. [20] 宋正平, 李畅, 孙灿辉. 克罗恩病肠腔纤维性狭窄的预测和影像学评估[J]. 影像诊断与介入放射学, 2020, 29(6): 445-50. https://www.cnki.com.cn/Article/CJFDTOTAL-YXZD202006008.htm [21] 徐锡涛, 冯琦, 周易, 等. 爬行脂肪组织在鉴别溃疡性结肠炎和克罗恩病中的应用[J]. 胃肠病学, 2018, 23(8): 455-60. https://www.cnki.com.cn/Article/CJFDTOTAL-WIEC201808002.htm [22] Kim YS, Kim SH, Ryu HS, et al. Iodine quantification on spectral detector-based dual-energy CT enterography: correlation with crohn's disease activity index and external validation[J]. Korean J Radiol, 2018, 19(6): 1077-88. [23] 郭淑栋, 张贝贝, 丁孝民, 等. MRI小肠造影可评估克罗恩病活动度分级及临床活动指数[J]. 分子影像学杂志, 2021, 44(4): 618-23. doi: 10.12122/j.issn.1674-4500.2021.04.09 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 249
- HTML全文浏览量: 85
- PDF下载量: 19
- 被引次数: 0