



Differential diagnosis of ductal breast cancer and intraductual papilloma by ultrasonography
-
摘要:
目的 探讨超声对导管型乳腺癌(DBC)与导管内乳头状瘤(IDP)患者的鉴别诊断。 方法 本研究为回顾性研究,以我院2017年1月~2020年12月收治的110例乳腺疾病患者作为研究对象,其中DBC患者59例,IDP患者51例,分析两组患者的常规超声、超声血流情况之间的差异,分析及Logistic回归诊断模型。 结果 IDP以及DBC患者的导管形态(χ2=25.692,P < 0.001)、导管走行(χ2=20.321,P < 0.001)、导管壁回声(χ2=6.052,P=0.014)及钙化灶情况(χ2=34.552,P < 0.001)的差异有统计学意义,两组患者的血流分布之间的差异有统计学意义(χ2=22.441,P < 0.001),但两组血流分级之间的差异无统计学意义(P>0.05);通过多因素分析,患者的导管、导管走行、导管壁回声、钙化、血流分布均是DBC诊断的重要因素。 结论 超声对DBC与IDP患者具有较强的鉴别诊断意义,导管增粗、导管走行不规则、导管壁回声不清晰、钙化不明显、血流分布均是DBC诊断的重要依据。 Abstract:Objective To explore the differential diagnosis between ductal breast cancer (DBC) and intraductual papilloma (IDP) by ultrasonography. Methods This retrospective study enrolled 110 patients with breast diseases treated in our hospital from January 2017 to December 2020. These patients included 59 patients with DBC and 51 patients with IDP. The differences of the routine ultrasound features and ultrasound blood flow between the two groups were compared.The logistic regression diagnostic model was analyzed. Results There were significant differences in the catheter morphology (χ2=25.692, P < 0.001), catheter running (χ2=20.321, P < 0.001), catheter wall echo (χ2=6.052, P=0.014), calcification foci (χ2=34.552, P < 0.001) and blood flow distribution (χ2=22.441, P < 0.001) between patients with IDP and DBC, while there was no significant difference in blood flow grade between the two groups (P>0.05). Through multivariate analysis, the patient's catheter, catheter running, catheter wall echo, calcification foci and blood flow distribution were important factors in the diagnosis of DBC. Conclusion Ultrasound has good differential diagnostic significance for patients with DBC and IDP. The thickening of catheter, irregular routing of catheter, unclear echo of catheter wall, unclear calcification foci and blood flow distribution are the important basis for the diagnosis of DBC. -
Key words:
- ductal breast cancer /
- intraductual papilloma /
- ultrasound /
- differential diagnosis
-

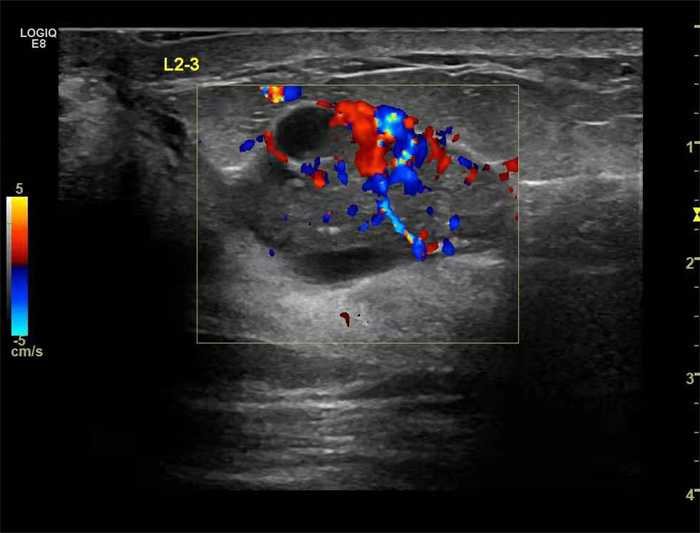
图 2 CDFI内测及条状血流信息
Figure 2. CDFI internal measurement and strip blood flow information.

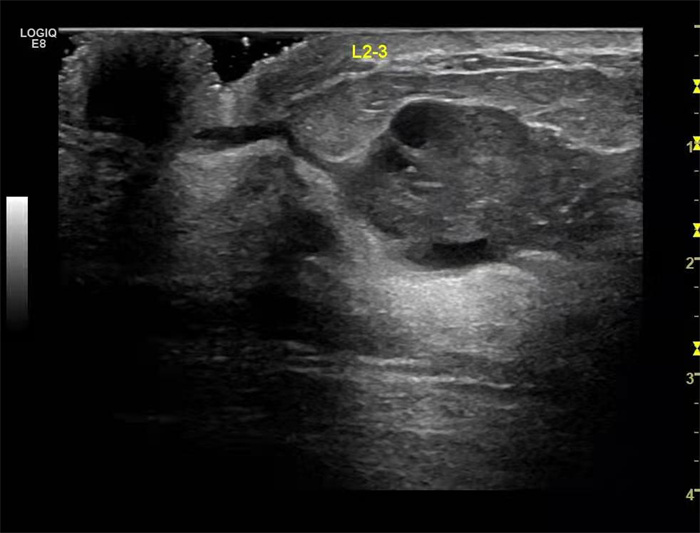
图 3 不规则低回声,边界清楚,内部回声不均匀,周边见扩张的导管样结构
Figure 3. Irregular low echo with clear boundary, uneven internal echo, and dilated ductlike structure around.

图 4 不规则低回声结构,边界不清,周边可以扩张的导管样结构
Figure 4. Irregular hypoechoic structures with ill-defined boundaries and circumferential ductlike structures.
表 1 两组患者一般资料比较
Table 1. Comparison of general data between the two groups (Mean±SD)
组别 年龄(岁) BMI(kg/m2) DBC组(n=59) 40.10±1.95 24.46±2.33 IDP组(n=51) 40.16±1.96 24.66±2.57 t 0.160 0.425 P 0.873 0.672 DBC: 导管型乳腺癌; IDP: 导管内乳头状瘤.  下载: 导出CSV
下载: 导出CSV
表 2 两组患者的常规超声指标分析
Table 2. Analysis of routine ultrasound indicators in the two groups [n(%)]
组别 导管增粗 导管走行不规则 导管壁回声不清晰 钙化灶 DBC(n=59) 36(61.02) 38(64.41) 37(62.71) 24(40.68) IDP(n=51) 7(13.73) 11(21.57) 20(39.22) 48(94.12) χ2 25.692 20.321 6.052 34.552 P < 0.001 < 0.001 0.014 < 0.001
下载: 导出CSV
表 3 两组患者的超声血流情况进行比较
Table 3. Comparison of ultrasonic blood flow between the two groups [n(%)]
组别 血流分级 血流分布 丰富 中等 无 导管周边 导管内部 周边及内部均可见 DBC(n=59) 12(20.34) 30(50.85) 17(28.81) 30(50.85) 6(10.17) 23(38.98) IDP(n=51) 8(15.69) 26(50.98) 17(33.33) 10(19.61) 25(49.02) 16(31.37) χ2 0.512 22.441 P 0.776 < 0.001
下载: 导出CSV
表 4 DBC诊断的多因素分析
Table 4. Multivariate analysis of DBC diagnosis
因素 β S.E. Wald P OR 95% CI 导管 0.339 2.360 1.320 < 0.001 1.022 0.900~1.931 导管走行 0.397 3.272 1.330 < 0.001 1.635 1.330~2.325 导管壁回声 0.007 3.293 1.330 < 0.001 1.606 1.390~2.315 钙化 0.541 3.225 1.452 lt; 0.001 1.442 1.211~1.590 血流分布 0.451 1.559 1.036 < 0.001 1.256 1.055~2.521
下载: 导出CSV
-
[1] Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CAACancer J Clin, 2021, 71(3): 209-49. doi: 10.3322/caac.21660 [2] Tasoulis MK, Lee HB, Yang W, et al. Accuracy of post-neoadjuvant chemotherapy image-guided breast biopsy to predict residual cancer [J]. JAMASurg, 2020, 155(12): e204103. [3] Demb J, Abraham L, Miglioretti DL, et al. Screening mammography outcomes: risk of breast cancer and mortality by comorbidity score and age[J]. J Natl Cancer Inst, 2020, 112(6): 599-606. doi: 10.1093/jnci/djz172 [4] 由秀, 许涛. 特殊类型乳腺癌的超声造影特征及其诊断价值研究[J]. 中国现代医学杂志, 2020, 30(20): 37-42. doi: 10.3969/j.issn.1005-8982.2020.20.008 [5] 钟雪仪, 邹绮嫦, 黄春兰. 超声对乳腺导管内乳头状瘤与肿块型导管内癌鉴别诊断价值[J]. 影像研究与医学应用, 2021, 5(11): 88-9, 92. doi: 10.3969/j.issn.2096-3807.2021.11.043 [6] 郭航, 邓晓妃, 方静, 等. 乳腺导管内原位癌与乳腺导管内乳头状瘤超声鉴别诊断logistic回归分析[J]. 广东化工, 2020, 47(7): 63-4, 70. doi: 10.3969/j.issn.1007-1865.2020.07.026 [7] Qian X, Pei J, Zheng H, et al. Prospective assessment of breast cancer risk from multimodal multiview ultrasound images via clinically applicable deep learning[J]. Nat Biomed Eng, 2021, 5(6): 522-32. doi: 10.1038/s41551-021-00711-2 [8] Henriksson A, Johansson B, Radu C, et al. Is it safe to exercise during oncological treatment? A study of adverse events during endurance and resistance training-data from the Phys-Can study[J]. Acta Oncol, 2021, 60(1): 96-105. doi: 10.1080/0284186X.2020.1851046 [9] Brogi E, Krystel-Whittemore M. Papillary neoplasms of the breast including upgrade rates and management of intraductal Papilloma without atypia diagnosed at core needle biopsy[J]. Mod Pathol, 2021, 34(suppl 1): 78-93. [10] Bhatnagar S, Bankar NG, Kulkarni MV, et al. Dissolvable microneedle patch containing doxorubicin and docetaxel is effective in 4T1 xenografted breast cancer mouse model[J]. Int J Pharm, 2019, 556: 263-75. doi: 10.1016/j.ijpharm.2018.12.022 [11] Cho N, Han W, Han BK, et al. Breast cancer screening with mammography plus ultrasonography or magnetic resonance imaging in women 50 years or younger at diagnosis and treated with breast conservation therapy[J]. JAMAOncol, 2017, 3(11): 1495-502. [12] Lee JM, Arao RF, Sprague BL, et al. Performance of screening ultrasonography as an adjunct to screening mammography in women across the spectrum of breast cancer risk[J]. JAMA Intern Med, 2019, 179(5): 658-67. doi: 10.1001/jamainternmed.2018.8372 [13] Sato K, Fuchikami H, Takeda N, et al. Validating the efficacy of single-stage breast-conserving therapy using multicatheter partialbreast brachytherapy based on updated ASTRO guidelines[J]. J Radiat Res, 2018, 59(3): 303-8. doi: 10.1093/jrr/rry033 [14] Jethwa KR, Kahila MM, Mara KC, et al. Patient-reported outcomes of catheter-based accelerated partial breast brachytherapy and whole breast irradiation, a single institution experience[J]. Breast Cancer Res Treat, 2018, 169(1): 189-96. doi: 10.1007/s10549-018-4665-6 [15] Strnad V, Major T, Polgar C, et al. ESTRO-ACROP guideline: Interstitial multi-catheter breast brachytherapy as Accelerated Partial Breast Irradiation alone or as boost-GEC-ESTRO Breast Cancer Working Group practical recommendations[J]. Radiother Oncol, 2018, 128(3): 411-20. doi: 10.1016/j.radonc.2018.04.009 [16] Weinstein SP, Korhonen K, Cirelli C, et al. Abbreviated breast magnetic resonance imaging for supplemental screening of women with dense breasts and average risk[J]. J Clin Oncol, 2020, 38(33): 3874-82. doi: 10.1200/JCO.19.02198 [17] Comstock CE, Gatsonis C, Newstead GM, et al. Comparison of abbreviated breast MRI vs digital breast tomosynthesis for breast cancer detection among women with dense breasts undergoing screening[J]. JAm MedAssoc, 2020, 323(8): 746-56. doi: 10.1001/jama.2020.0572 [18] Kumar S, Sharife H, Kreisel T, et al. Intra-tumoral metabolic zonation and resultant phenotypic diversification are dictated by blood vessel proximity[J]. Cell Metab, 2019, 30(1): 201-11. e6. doi: 10.1016/j.cmet.2019.04.003 [19] Zhao R, Wang B, Yang X, et al. A drug-free tumor therapy strategy: cancer-cell-targeting calcification[J]. Angew Chem Int Ed Engl, 2016, 55(17): 5225-9. doi: 10.1002/anie.201601364 [20] Conti A, Duggento A, Indovina I, et al. Radiomics in breast cancer classification and prediction[J]. SeminCancerBiol, 2021, 72: 238-50. -


 点击查看大图
点击查看大图

计量
- 文章访问数: 282
- HTML全文浏览量: 124
- PDF下载量: 13
- 被引次数: 0