



Diagnosis and risk stratification of pulmonary embolism by dual-energy CT perfusion
-
摘要:
目的 探讨双能量CT肺灌注的灌注缺陷对肺栓塞诊断及危险分层。 方法 选取我院2018年1月~2020年12月157例临床疑诊为肺栓塞的患者为研究对象,最终120例患者确诊肺栓塞,所有患者均行双能量CT肺灌注成像(DEPI)及肺动脉CT血管造影成像(CTPA),根据临床生物学标志及影像学改变,将患者分为肺栓塞低危组(n=30)、中危组(n=35)、高危组(n=55)。比较患者肺栓塞数量,肺动脉灌注缺失面积分数、右/左心室短轴最大径比值及心脏生物学标志物。所有患者随访3月并记录结局。 结果 DEPI与CTPA对肺栓塞的诊断相符,诊断符合率为86.1%; CTPA和DEPI联合诊断的曲线下面积为0.95,特异性为89.20%,敏感度为95.80%,Youden指数为0.85,较CTPA和DEPI单独诊断肺栓塞更好。肺栓塞低危组、中危组、高危组的灌注缺损面积、心脏生物学标志物及右/左心室短轴最大径比值经两两比较差异有统计学意义(P < 0.05)。 结论 DEPI可作为CTPA的诊断肺栓塞的补充,并通过肺动脉灌注缺失面积分数危险分层,是一种新的临床诊疗方案的选择。 Abstract:Objective To investigate the role of perfusion defects in dual-energy CT pulmonary perfusion in the diagnosis and risk stratification of pulmonary embolism. Methods A total of 157 patients diagnosed with suspected pulmonary embolism in our hospital from January 2018 to December 2020 were enrolled, and pulmonary embolism was finally confirmed in 120 patients. All patients were performed with dual- energy CT pulmonary perfusion imaging (DEPI) and pulmonary artery CT angiography (CTPA). The number of pulmonary embolisms, pulmonary artery loss area fraction, right/left ventricular short-axis maximum diameter ratio and cardiac biological markers were recorded and compared. All patients were followed up for 3 months with the outcomes recorded. Results Dual-energy CT was consistent with CTPA in the diagnosis of pulmonary embolism, with a diagnostic coincidence rate of 86.1%. For CTPA combined with DEPI, AUC value was 0.95, with the specificity, sensitivity, and Youden index of 89.20%, 95.80% and 0.85, respectively, better than CTPA and DEPI alone in the diagnosis of pulmonary embolism. There were significant differences in perfusion defect area, cardiac biological markers, and right/left ventricular short- axis maximum diameter ratio levels between the low-risk, medium-risk, and high- risk groups of pulmonary embolism (P < 0.05). Conclusion DEPI can be used as a supplement for the diagnosis of pulmonary embolism by CTPA. Through risk stratification for pulmonary artery perfusion loss area fraction, it is a new option for clinical diagnosis and treatment, suitable for clinical promotion. -

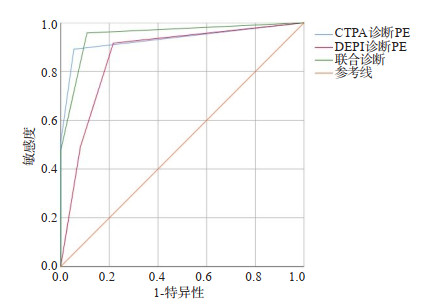
图 1 CTPA与DEPI对PE患者诊断严重程度的ROC曲线
Figure 1. ROC curve of CTPA and DEPI on the diagnostic severity of PE patients.

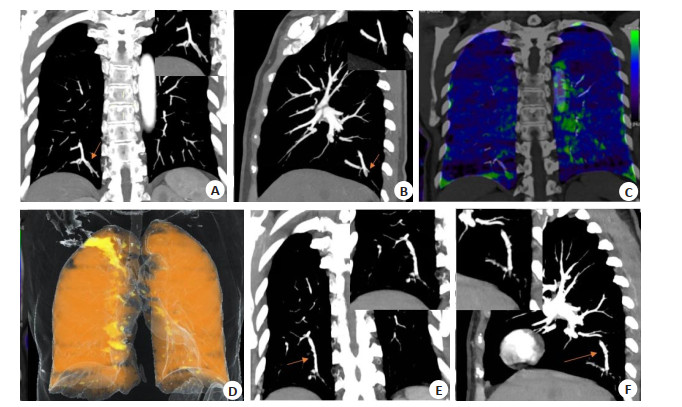
图 2 低危组女性患者,72岁
A~B: 右肺下叶后基底段动脉栓塞; C~D: 未出现明显的灌注缺失, 灌注缺失面积小; E~F: 治疗后复查预后良好, 原右肺下叶后基底段栓塞动脉复通.
Figure 2. Low risk group: a 72-year-old female patient.

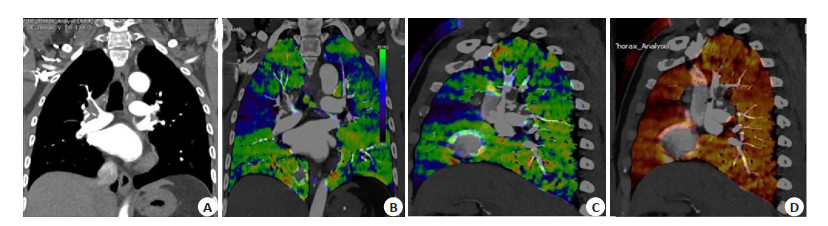
图 3 PAOI高危组男性患者,60岁,诊断为肺动脉主干及肺叶分支栓塞
A: MPR冠状位显示左右肺动脉主干及分支肺栓塞; B~C: 肺灌注冠矢状位左右肺动脉栓塞供血区域显示蓝色灌注缺失; D: 双能量融合图中肺栓塞区域同样灌注缺失, 灌注缺失占比面积较大, 故该患者在随访中死亡.
Figure 3. PAOI high-risk group: A60-year-old male patient, diagnosed with embolism of the main pulmonary artery and lobe branches.
表 1 DEPI与CTPA诊断PE的结果
Table 1. Results of DEPI and CTPA in the diagnosis of PE (n)
DEPI CTPA 合计 无栓塞 部分栓塞 完全栓塞 灌注无异常 1645 102 45 1792 灌注部分缺损 62 712 92 866 灌注完全缺损 54 39 93 186 总计 1761 853 230 2844 DEPI: 双能量CT肺灌注成像; CTPA: 肺动脉CT血管造影.  下载: 导出CSV
下载: 导出CSV
表 2 CTPA与DEPI对PE患者诊断的比较
Table 2. Comparison between TPA and DEPI in the diagnosis of PE patients [n(%)]
诊断方法 确诊有无肺栓塞 χ2 P 无 有 CTPA诊断PE 93.74 < 0.001 无栓塞 35(72.9) 13(27.1) 部分栓塞 2(4.2) 46(95.8) 完全栓塞 0(0.0) 61(100.0) DEPI诊断PE 74.59 < 0.001 无灌注缺失 29(74.4) 10(25.6) 部分灌注缺失 5(8.9) 51(91.1) 完全灌注缺失 3(4.8) 59(95.2) 联合诊断 96.03 < 0.001 无栓塞 32(80.0) 8(20.0) 部分栓塞 5(8.3) 55(91.7) 完全栓塞 0(0.0) 57(100.0)
下载: 导出CSV
表 3 CTPA与DEPI对PE患者诊断的ROC曲线分析
Table 3. ROC curve analysis of CTPA and depi in the diagnosis of PE patients
项目 AUC SE P 95% CI 特异性(%) 敏感度(%) Youden指数 CTPA 0.93 0.02 < 0.001 0.89~0.97 96.60 89.20 0.83 DEPI 0.87 0.04 < 0.001 0.79~0.94 78.40 91.70 0.70 联合诊断 0.95 0.01 < 0.001 0.91~0.98 89.20 95.80 0.85
下载: 导出CSV
表 4 肺栓塞患者各组栓塞灌注缺损面积、BNP及RV/LV的比较
Table 4. Comparison of embolism perfusion defect area, BNP and RV/LV in each group of patients with pulmonary embolism
组别 灌注缺损面积(%) BNP(pg/mL) RV/LV 低危组(n=30) 7.04±0.99 155.10±41.54 0.85±0.15 中危组(n=35) 34.80±1.57a 423.03±22.75a 0.99±0.09a 高危组(n=55) 65.05±10.32ab 2126.22±263.86ab 1.33±0.05ab Z 103.89 83.77 96.77 P < 0.001 < 0.001 < 0.001 aP < 0.05 vs低危组, bP < 0.05 vs中危组.
下载: 导出CSV
-
[1] 王利, 刘绍霞. 急性肺栓塞患者血清BNP、TnI及Hcy水平变化及临床意义[J]. 川北医学院学报, 2021, 36(5): 652-4. doi: 10.3969/j.issn.1005-3697.2021.05.027 [2] Barrera CA, Otero HJ, Fenlon EP 3rd, et al. CTA utilization for evaluation of suspected pulmonary embolism in a tertiary pediatric emergency department[J]. Clin Imaging, 2021, 75: 105-10. doi: 10.1016/j.clinimag.2020.12.024 [3] 高洪媛, 李兆立, 邹新华. 双源CT flash扫描模式在自由呼吸状态下肺动脉成像的可行性探讨[J]. 中国CT和MRI杂志, 2020, 18(2): 26-8. doi: 10.3969/j.issn.1672-5131.2020.02.009 [4] Perez-Johnston R, Plodkowski AJ, Halpenny DF, et al. Perfusion defects on dual-energy CTA in patients with suspected pulmonary embolism correlate with right heart strain and lower survival[J]. Eur Radiol, 2021, 31(4): 2013-21. doi: 10.1007/s00330-020-07333-3 [5] 许令荣, 赵卉, 刘云峰, 等. CT肺动脉栓塞指数(PAOI)和PESI评分对急性肺栓塞预后评价中的作用[J]. 临床肺科杂志, 2019, 24(6): 981-4. doi: 10.3969/j.issn.1009-6663.2019.06.004 [6] 中华医学会呼吸病学分会肺栓塞与肺血管病学组, 中国医师协会呼吸医师分会肺栓塞与肺血管病工作委员会, 全国肺栓塞与肺血管病防治协作组. 肺血栓栓塞症诊治与预防指南[J]. 中华医学杂志, 2018, 98(14): 1060-87. doi: 10.3760/cma.j.issn.0376-2491.2018.14.007 [7] 焦亚彬, 耿园园, 李培秀, 等. 双源CT肺动脉造影及肺灌注成像对肺栓塞治疗后效果评价[J]. 临床肺科杂志, 2018, 23(2): 288-91. doi: 10.3969/j.issn.1009-6663.2018.02.026 [8] 黄玉芳, 龙瀛, 欧国春, 等. IMA、IL-38、DFR水平与急性肺栓塞患者危险分层和预后的相关性[J]. 中南医学科学杂志, 2022, 50(2): 219- 22. https://www.cnki.com.cn/Article/CJFDTOTAL-HYYY202202015.htm [9] 郑静. 溶栓联合抗凝治疗次大面积肺栓塞患者的效果及安全性分析[J]. 健康研究, 2019, 39(2): 212-5. doi: 10.3969/j.issn.1674-6449.2019.02.026 [10] Gjonbrataj E, Kim JN, Gjonbrataj J, et al. Risk factors associated with provoked pulmonary embolism[J]. Korean J Intern Med, 2017, 32(1): 95-101. doi: 10.3904/kjim.2015.118 [11] E. K. Weidman, A. J. Plodkowski, D. F. Halpenny, 等. 双能量CT血管成像检测肺栓塞: 碘图的附加益处[J]. 国际医学放射学杂志, 2019, 42(1): 109. https://www.cnki.com.cn/Article/CJFDTOTAL-GWLC201901044.htm [12] Geyer LL, Scherr M, Körner M, et al. Imaging of acute pulmonary embolism using a dual energy CT system with rapid kVp switching: initial results[J]. Eur J Radiol, 2012, 81(12): 3711-8. doi: 10.1016/j.ejrad.2011.02.043 [13] 郭小皖, 孙吉林, 兰艳芹, 等. 双源CT冠脉成像安全辐射剂量与图像质量研究[J]. 川北医学院学报, 2018, 33(2): 235-8. doi: 10.3969/j.issn.1005-3697.2018.02.024 [14] 韩雪, 张晓琴. 双源CT肺灌注成像评估肺血栓栓塞症的研究进展[J]. 内蒙古医学杂志, 2019, 51(5): 527-30. https://www.cnki.com.cn/Article/CJFDTOTAL-NMYZ201905007.htm [15] 耿会霞, 张万春, 安彩霞, 等. 肺通气灌注联合肺灌注融合断层显像与CT肺动脉造影对肺栓塞诊断价值的比较[J]. 中国医师杂志, 2019, 21(7): 1020-3, 1029. doi: 10.3760/cma.j.issn.1008-1372.2019.07.014 [16] 梁田, 刘会, 谢晟, 等. 肺动脉CTA漏诊亚段肺栓塞原因分析[J]. 中国医学影像技术, 2018, 34(8): 1220-3. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYXX201808034.htm [17] Thieme SF, Graute V, Nikolaou K, et al. Dual Energy CT lung perfusion imaging-Correlation with SPECT/CT[J]. Eur J Radiol, 2012, 81(2): 360-5. doi: 10.1016/j.ejrad.2010.11.037 [18] 许令荣. 肺栓塞指数(PAOI)联合心脏彩超、PESI评分对急性肺栓塞严重程度及预后评价中的作用[D]. 合肥: 安徽医科大学, 2019. [19] 奚泉, 赵春林, 刘娜. 大面积肺栓塞患者CT肺动脉栓塞指数与心血管参数的相关性研究[J]. 中国医学装备, 2021, 18(4): 70-3. doi: 10.3969/J.ISSN.1672-8270.2021.04.017 [20] 富青, 杨明, 雷子乔, 等. 基于第3代双源CT双低检查技术在肺栓塞成像的临床应用研究[J]. 中华放射医学与防护杂志, 2020, 40(9): 712-6. doi: 10.3760/cma.j.issn.0254-5098.2020.09.011 [21] Moore AJE, Wachsmann J, Chamarthy MR, et al. Imaging of acute pulmonary embolism: an update[J]. Cardiovasc Diagn Ther, 2018, 8 (3): 225-43. doi: 10.21037/cdt.2017.12.01 [22] Ende-Verhaar YM, Kroft LJM, Mos ICM, et al. Accuracy and reproducibility of CT right-to-left ventricular diameter measurement in patients with acute pulmonary embolism[J]. PLoS One, 2017, 12 (11): e0188862. doi: 10.1371/journal.pone.0188862 [23] 李雅敏, 米玉红, 陆艳辉, 等. 残余血栓对右心功能不全的急性肺栓塞患者远期预后的影响[J]. 心肺血管病杂志, 2021, 40(4): 330-5. doi: 10.3969/j.issn.1007-5062.2021.04.006 [24] 虎义科, 赵蓉, 张广浩, 等. 256层螺旋CT肺动脉造影对肺动脉栓塞患者右心功能的评价[J]. 罕少疾病杂志, 2022, 29(3): 46-7, 53. https://www.cnki.com.cn/Article/CJFDTOTAL-HSJB202203018.htm -

 点击查看大图
点击查看大图
计量
- 文章访问数: 512
- HTML全文浏览量: 143
- PDF下载量: 7
- 被引次数: 0