



Effect of laparoscopic pancreaticoduodenectomy for pancreatic head malignant tumor and imaging analysis of pancreas before and after operation
-
摘要:
目的 探讨腹腔镜胰十二指肠切除术对治疗胰头恶性肿瘤的效果,分析手术前后胰腺影像学特点。 方法 选取本院2020年1月~2021年6月收治的胰头恶性肿瘤患者110例,按手术方法的不同将患者分为两组,观察组:采用腹腔镜十二指肠切除术(n=61); 对照组:采用开腹十二指肠切除术(n=49)。分析两组患者围手术期指标、手术切除的完整性、炎性反应,并发症的发生率、术前与术后胰腺影像学特点。 结果 两组患者手术时间、手术切除的完整性及并发症的发生率差异无统计学意义(P > 0.05),观察组术中出血量和住院时间均低于对照组,差异有统计学意义(P < 0.05); 观察组血清C-反应蛋白、白介素-6、肿瘤坏死因子-α水平低于对照组(P < 0.05); 术前CT显示胰头部可见不规则囊状低密度影,边缘分叶、内分隔、密度欠均匀,增强边界较清楚,术后有患者可见术区范围包裹性积液、局部密度稍高。 结论 腹腔镜胰十二指肠切除术治疗胰头恶性肿瘤可以减轻机体炎性反应,降低术中出血和缩短住院时间,其手术切除的完整性与开腹手术相当,且借助CT术前影像能有效指导手术过程和识别术后胰瘘等并发症。 Abstract:Objective To investigate the effect of laparoscopic pancreaticoduodenectomy in the treatment of pancreatic head malignant tumor, and analyze the imaging characteristics of pancreas before and after operation. Methods A total of 110 patients with pancreatic head malignant tumor treated in our hospital from January 2020 to June 2021 were selected. They were divided into 2 groups according to different surgical methods. Among them, 61 patients in the observation group were treated with laparoscopic duodenectomy, and 49 patients in the control group were treated with open duodenectomy. Perioperative indicators, surgical integrity and inflammatory response of patients in the two groups were observed. The incidence of complications, preoperative and postoperative pancreatic imaging characteristics were analyzed. Results There were no statistically significant differences in the operative time, the completeness of surgical resection and the incidence of complications between the two groups (P > 0.05). The amount of intraoperative blood loss and length of hospital stay were significantly shorter than those in the control group, with statistically significant differences (P < 0.05). The serum levels of C-reactive protein, IL-6 and TNF-α in observation group were significantly lower than those in control group (P < 0.05). Preoperative CT showed irregular cystic low-density shadow on the head of the pancreas, with lobed edges, internal separation, uneven density and clear enhanced boundary. After surgery, patients had encapsulated effusion in the operation area and slightly higher local density. Conclusion Laparoscopic pancreaticoduodenectomy in the treatment of pancreatic head malignant tumor can reduce inflammatory response, reduce intraoperative bleeding and shorten hospital stay. The integrity of surgical resection is similar to that of open surgery, and the preoperative CT images can effectively guide the surgical process and identify postoperative pancreatic fistula and other complications. -

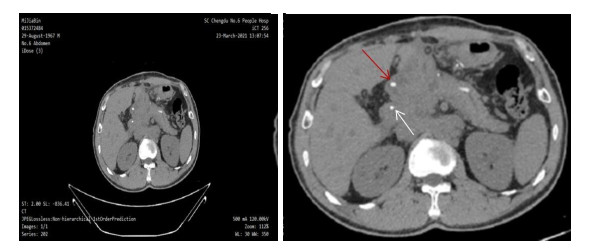
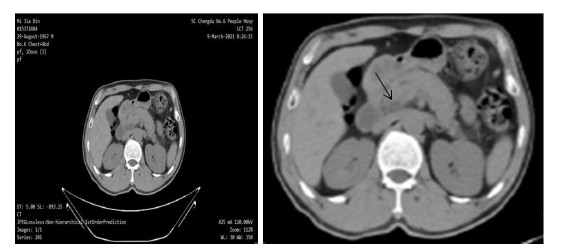
图 1 胰头肿瘤术前CT平扫影像(黑箭所指为肿瘤,灰黑色)
Figure 1. Preoperative CT images of pancreatic head carcinoma.

图 2 胰十二指肠切除术术后CT影像
术后: 胰十二指肠切除术后腹部CT平扫复查, 术区范围包裹性积液,局部密度稍高; 胆总管、胰管内见置管, 十二指肠肿胀. 图中红箭所指(高密度影,白色)为胰管置管, 白箭所指为胆管置管(高密度影, 白色).
Figure 2. CT images after pancreaticoduodenectomy
表 1 两组患者围手术期指标比较
Table 1. Comparison of perioperative indexes between the two groups (Mean±SD)
组别 手术时间(min) 术中出血量(mL) 住院时间(d) 观察组(n=61) 281.33±38.15 205.25±40.28 11.35±3.05 对照组(n=49) 267.53±41.24 285.38±72.54 15.25±3.35 t 1.819 7.338 6.379 P 0.072 < 0.001 < 0.001  下载: 导出CSV
下载: 导出CSV
表 2 两组患者手术切除的完整性比较
Table 2. Comparison of surgical resection integrity between the two groups [n(%)]
组别 R0 R1 R2 观察组(n=61) 53(86.89) 6(9.84) 2(3.28) 对照组(n=49) 42(85.71) 5(10.20) 2(4.08) Z 0.035 P 0.852
下载: 导出CSV
表 3 两组患者炎性因子水平比较
Table 3. Comparison of inflammatory factors between the two groups (Mean±SD)
组别 CRP(mg/L) IL-6(ng/L) TNF-α(ng/L) 术前 术后 术前 术后 术前 术后 观察组(n=61) 14.52±3.14 72.27±15.21* 12.25±3.37 44.68±6.84* 96.25±15.34 173.28±29.75* 对照组(n=49) 15.83±4.87 96.35±18.59* 11.57±2.81 59.17±9.58* 94.86±16.05 194.37±38.24* t 1.706 7.473 1.131 9.243 0.463 3.254 P 0.091 < 0.001 0.261 < 0.001 0.645 0.002 *P < 0.05 vs同组术前. CRP: C-反应蛋白; IL-6: 白介素-6; TNF-α: 肿瘤坏死因子-α.
下载: 导出CSV
表 4 两组患者术后并发症发生率比较
Table 4. Comparison of postoperative complications between the two groups [n(%)]
组别 出血 感染 胰瘘 胆瘘 胃肠吻合口瘘 胃排空功能障碍 总发生率 观察组(n=61) 2(3.28) 1(1.64) 2(3.28) 0(0) 3(4.92) 4(6.56) 12(19.67) 对照组(n=49) 3(60.12) 2(4.08) 2(4.08) 1(2.04) 0(0) 2(4.08) 10(20.41) χ2 0.009 P 0.924
下载: 导出CSV
-
[1] McGuigan A, Kelly P, Turkington RC, et al. Pancreatic cancer: a review of clinical diagnosis, epidemiology, treatment and outcomes[J]. World J Gastroenterol, 2018, 24(43): 4846-61. doi: 10.3748/wjg.v24.i43.4846 [2] 吴伟顶. 腹腔镜技术在胰腺恶性肿瘤中的应用[J]. 肝胆胰外科杂志, 2020, 32(5): 261-4. https://www.cnki.com.cn/Article/CJFDTOTAL-GDYW202005003.htm [3] Aguilera F, Tsamalaidze L, Raimondo M, et al. Pancreatico-duodenectomy and outcomes for groove pancreatitis[J]. Dig Surg, 2018, 35(6): 475-81. doi: 10.1159/000485849 [4] Lyu YX, Cheng YX, Wang B, et al. Minimally invasive versus open pancreaticoduodenectomy: an up-to-date meta-analysis of comparative cohort studies[J]. J Laparoendosc Adv Surg Tech A, 2019, 29(4): 449-57. doi: 10.1089/lap.2018.0460 [5] Kawai M, Hirano S, Yamaue H. Artery-first approach for pancreaticoduodenectomy[J]. J Hepatobiliary Pancreat Sci, 2018, 25 (6): 319-20. doi: 10.1002/jhbp.554 [6] Xiang YE, Wu JC, Lin C, et al. Pancreatic reconstruction techniques after pancreaticoduodenectomy: a review of the literature[J]. Expert Rev Gastroenterol Hepatol, 2019, 13(8): 797-806. doi: 10.1080/17474124.2019.1640601 [7] 陈汝福, 钟诚锐, 周泉波. 胰头癌微创手术治疗的现状及展望[J]. 临床肝胆病杂志, 2019, 35(5): 953-7. doi: 10.3969/j.issn.1001-5256.2019.05.004 [8] 刘学青, 王朝龙, 冯峰, 等. 腹腔镜胰十二指肠切除术治疗胰头癌57例疗效[J]. 中华肝胆外科杂志, 2019, 25(7): 521-5. doi: 10.3760/cma.j.issn.1007-8118.2019.07.010 [9] 潘国宗. 中华医学百科全书: 消化病学[M]. 北京: 中国协和医科大学出版社, 2015. [10] 戴梦华. 腹腔镜胰十二指肠切除术R0切除技巧[J]. 中国实用外科杂志, 2018, 38(7): 824-5. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGWK201807031.htm [11] Nieuwenhuijs VB, de Klein GW, van Duijvendijk P, et al. Lessons learned from the introduction of laparoscopic pancreatico-duodenectomy[J]. J Laparoendosc Adv Surg Tech A, 2020, 30(5): 495-500. doi: 10.1089/lap.2019.0695 [12] del Chiaro M, Valente R, Arnelo U. Minimally invasive pancreatico-duodenectomy for the treatment of pancreatic- head and periampullary tumors[J]. JAMA Surg, 2017, 152(4): 343. doi: 10.1001/jamasurg.2016.4754 [13] 金巍巍, 徐晓武, 牟一平, 等. 腹腔镜胰十二指肠切除术单中心233例临床经验总结[J]. 中华外科杂志, 2017, 55(5): 354-8. doi: 10.3760/cma.j.issn.0529-5815.2017.05.009 [14] 刘学青, 邢中强, 秦建章, 等. 腹腔镜胰十二指肠切除术单中心300例临床分析[J]. 中国实用外科杂志, 2018, 38(3): 306-11. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGWK201803020.htm [15] 陈志诚, 刘军. 腹腔镜胰十二指肠切除术的应用现状及展望[J]. 临床肝胆病杂志, 2018, 34(9): 2027-32. doi: 10.3969/j.issn.1001-5256.2018.09.042 [16] 郑卫华, 孟兴凯, 任建军, 等. 腹腔镜胰十二指肠切除术安全性及有效性初探[J]. 肝胆胰外科杂志, 2021, 33(3): 165-9. https://www.cnki.com.cn/Article/CJFDTOTAL-GDYW202103010.htm [17] 于洪武, 张芸, 代伟, 等. 基层医院腹腔镜胰十二指肠切除术的学习曲线[J]. 肝胆胰外科杂志, 2021, 33(4): 240-2. https://www.cnki.com.cn/Article/CJFDTOTAL-GDYW202104014.htm [18] 马春阳, 朱峰, 王敏, 等. 腹腔镜胰十二指肠切除术合并扩大淋巴结清扫治疗胰头癌的临床疗效分析[J]. 外科理论与实践, 2017, 22(2): 117-22. https://www.cnki.com.cn/Article/CJFDTOTAL-WKLL201702010.htm [19] 纪明哲, 韦荣强, 陈丹磊, 等. 整块切除在胰头癌根治术中应用进展[J]. 中国实用外科杂志, 2019, 39(7): 741-3. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGWK201907032.htm [20] Leeuw D, Pranger BK, de Jong KP, et al. Routine chest computed tomography for staging of pancreatic head carcinoma[J]. Pancreas, 2020, 49(3): 387-92. doi: 10.1097/MPA.0000000000001494 [21] Prochazka V, Hlavsa J, Kunovsky L, et al. Correlation of survival length after pancreaticoduodenectomy for pancreatic head adenocarcinoma depending on tumor characteristics detected by means of computed tomography and resection margins status[J]. Neoplasma, 2020, 67(6): 1319-28. [22] Tonolini M, Ierardi AM, Carrafiello G. Elucidating early CT after pancreatico-duodenectomy: a primer for radiologists[J]. Insights Imaging, 2018, 9(4): 425-36. doi: 10.1007/s13244-018-0616-3 [23] Quesada R, Simón C, Radosevic A, et al. Morphological changes of the pancreas after pancreaticoduodenectomy[J]. Sci Rep, 2019, 9(1): 14517. doi: 10.1038/s41598-019-51173-1 [24] Ohgi K, Okamura Y, Sugiura T, et al. Pancreatic attenuation on computed tomography predicts pancreatic fistula after pancreatico-duodenectomy[J]. HPB (Oxford), 2020, 22(1): 67-74. doi: 10.1016/j.hpb.2019.05.008 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 186
- HTML全文浏览量: 74
- PDF下载量: 1
- 被引次数: 0