



Relationship between spiral CT perfusion parameters and C-reactive protein, procalcitonin, serum amylase, hematocrit and clinical symptoms in patients with severe pancreatitis
-
摘要:
目的 研究重症胰腺炎患者螺旋CT灌注参数与炎症指标C反应蛋白、降钙素原、血清淀粉酶、红细胞积压及临床症状的关系。 方法 回顾性收集2019年1月~2021年1月我院收治的102例胰腺炎患者临床资料,根据Ranson评分将患者分为轻症组(n=64,Ranson评分 < 3分)和重症组(n=38,Ranson评分3~11分)。统计两组炎症指标、临床症状评分及CT关注参数,采用Pearson相关性分析CT灌注参数与炎症指标、临床症状的相关性。 结果 重症组血清C反应蛋白、降钙素原、血清淀粉酶水平及外周血红细胞积压水平、Ranson、急性生理与慢性健康评分(APACHE-Ⅱ)高于轻症组(P < 0.05),血流量、血流容积低于轻症组(P < 0.05)。Pearson相关性分析结果显示,血流量、血流容积与外周血红细胞积压水平及Ranson、APACHE-Ⅱ评分呈负相关(r=-0.632、-0.673、-0.703和-0.715、-0.662、-0.637,P < 0.05)。 结论 胰腺炎患者病情加重血清C反应蛋白、降钙素原、血清淀粉酶水平及外周血红细胞积压水平,Ranson、APACHE-Ⅱ评分升高,血流量、血流容积降低,重症胰腺炎患者血流量、血流容积与外周血红细胞积压水平、Ranson、APACHE-Ⅱ评分呈显著负相关关系。 Abstract:Objective To explore the relationship between perfusion parameters of spiral CT and C-reactive protein, procalcitonin, serum amylase, hematocrit and clinical symptoms in patients with severe pancreatitis. Methods Clinical data of 102 patients with pancreatitis admitted to our hospital from January 2019 to January 2021 were retrospectively collected. The patients were divided into the mild group (n=64, score of Ranson < 3 points) and the severe group (n=38, score of Ranson 3-11 points) according to Ranson score. The inflammatory indicators, score of clinical symptom and CT concern parameters of the two groups were statistically analyzed, and the correlation between CT perfusion parameters and inflammatory indicators and clinical symptoms was analyzed by Pearson correlation. Results The levels of serum C-reactive protein, procalcitonin, serum amylase, peripheral blood hematocrit and scores of Ranson, acute physiology and chronic health score (APACHE- II) in the severe group were higher than those in the mild group (P < 0.05), while blood flow, blood flow volume were lower than those in the mild group (P < 0.05). Pearson correlation analysis showed that blood flow and blood flow volume were significantly negatively correlated with level of peripheral blood hematocrit, scores of Ranson and APACHE-II (r=-0.632, -0.673, -0.703 and -0.715, -0.662, -0.637, P < 0.05). Conclusion The levels of serum C-reactive protein, procalcitonin and serum amylase, peripheral blood hematocrit, scores of Ranson and APACHE- II are increased, while blood flow and blood flow volume decreased in patients with severe pancreatitis. Blood flow and blood flow volume are significantly negatively correlated with level of peripheral blood hematocrit, scores of Ranson and APACHE-II. -
Key words:
- pancreatitis /
- severe /
- computed tomography /
- C-reactive protein /
- procalcitonin /
- serum amylase /
- hematocrit /
- clinical symptoms
-

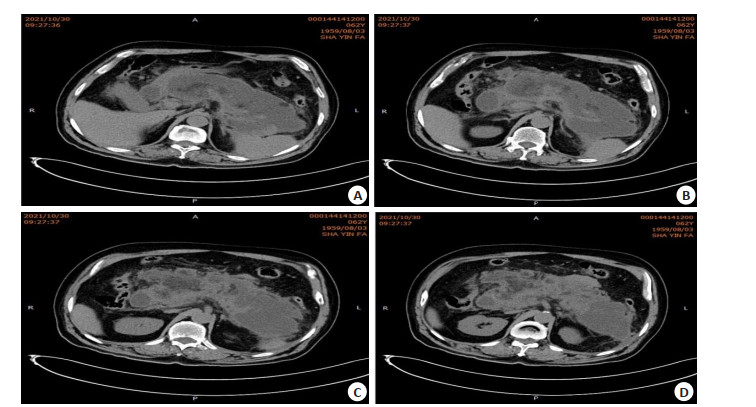
图 1 典型病例1,62岁男性,突发恶心、呕吐伴上腹部疼痛18 h入院
A: 胰腺弥漫性增大, 实质不均匀密度减低, 周围间隙及双侧肾前间隙渗出、积液, 局部见小斑片状脂肪密度, 考虑急性胰腺炎可能, 较前片周围渗出稍减少; B: 胆囊张力增高; C~D: 腹腔散在小淋巴结影.
Figure 1. Typical case 1, a 62- year- old male patient, was hospitalized for 18 h with sudden nausea and vomiting and upper abdominal pain.

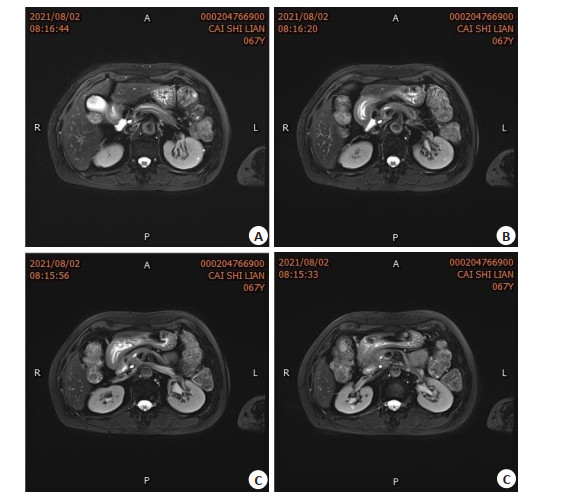
图 2 典型病例2,67岁女性,因腹痛超过6 d入院
A: 肝脏形态、大小未见异常, 左肝内叶可见类圆形长T2、长T1信号小结节样影, DWI呈高信号, 反相位未见肝实质信号降低, 增强扫描结节呈明显稍高信号强化; 胆囊不大, 壁不厚, 其内未见异常信号; B: 胰腺不大, 信号均匀, 所见腹侧及背侧胰管未见融合, 胰头区可见胰管分别开口于十二指肠降段, 增强扫描胰腺未见明显异常强化灶, 所见十二指肠乳突增大, 呈稍长T2、长T1信号,增强扫描,动脉期及门静脉期呈低信号, 延迟扫描呈等信号; C: 脾脏前缘可见类圆形长T2、短T1信号结节样影,增强扫描未见明显强化; 腹腔及腹膜后未见淋巴结肿大; D: 所见双肾可见类圆形长T2信号影, 增强扫描未见明显强化.
Figure 2. Typical case 2, a 67-year-old female patient was hospitalized with abdominal pain for more than 6 d.
表 1 两组炎症指标比较
Table 1. Comparison of inflammatory indexes between two groups (Mean±SD)
组别 CRP(U/L) PCT(μg/L) S-Amy(U/L) HCT(%) 轻症组(n=64) 81.26±9.27 1.63±0.73 804.27±23.74 34.83±5.64 重症组(n=38) 156.37±13.27 3.96±0.99 996.37±53.72 46.37±7.25 t 46.912 13.439 24.706 8.845 P < 0.001 < 0.001 < 0.001 < 0.001 CRP: C反应蛋白; PCT: 降钙素原; S-Amy: 血清淀粉酶; HCT: 红细胞积压.  下载: 导出CSV
下载: 导出CSV
表 2 两组临床症状评分比较
Table 2. Comparison of clinical symptom scores between two groups (score, Mean±SD)
组别 Ranson评分 APACHE-Ⅱ评分 轻症组(n=64) 1.83±0.29 2.07±0.89 重症组(n=38) 4.27±1.71 15.37±3.28 t 11.175 30.604 P < 0.001 < 0.001
下载: 导出CSV
表 3 两组CT灌注参数比较
Table 3. Comparison of CT perfusion parameters between two groups (Mean±SD)
组别 MTT(s) BF(100 mL·min) PS[0.5 mL/(100 mL·min)] BV(mL/1) 轻症组(n=64) 8.50±1.22 132.37±19.27 117.84±23.84 177.36±21.37 重症组(n=38) 8.55±1.36 78.37±9.37 114.38±24.63 106.36±17.84 t 0.189 27.853 0.688 16.888 P 0.851 < 0.001 0.493 < 0.001 MTT: 灌注起始时间; BF: 血流量; PS: 血液流速; BV: 血流容积.
下载: 导出CSV
表 4 CT灌注参数与炎症指标、临床症状的相关性分析
Table 4. Correlation analysis of CT perfusion parameters with inflammatory indexes and clinical symptoms
CT灌注参数 S-Amy PCT CRP HCT Ranson评分 APACHE-Ⅱ评分 r P r P r P r P r P r P BF -0.308 > 0.05 -0.042 > 0.05 -0.152 > 0.05 -0.632 < 0.05 -0.673 < 0.05 -0.703 < 0.05 BV -0.232 > 0.05 -0.062 > 0.05 -0.093 > 0.05 -0.715 < 0.05 -0.662 < 0.05 -0.637 < 0.05
下载: 导出CSV
-
[1] Singh VK, Yadav D, Garg PK. Diagnosis and management of chronic pancreatitis: a review[J]. JAMA, 2019, 322(24): 2422-34. doi: 10.1001/jama.2019.19411 [2] 赵瑞臣, 次多, 何春娅, 等. 重症急性胰腺炎外周血miR-9、miR-155表达水平与淀粉酶、炎性反应及Th17/Treg平衡的关系[J]. 疑难病杂志, 2021, 20(8): 795-800. doi: 10.3969/j.issn.1671-6450.2021.08.009 [3] 何文华, 郑西, 祝荫, 等. 基于大样本数据库比较APACHE Ⅱ、Ranson、BISAP和CTSI评分在早期预测急性胰腺炎病情严重程度的价值[J]. 中华胰腺病杂志, 2019, 19(3): 172-6. doi: 10.3760/cma.j.issn.1674-1935.2019.03.004 [4] Fung C, Svystun O, Fouladi DF, et al. CT imaging, classification, and complications of acute pancreatitis[J]. Abdom Radiol (NY), 2020, 45 (5): 1243-52. doi: 10.1007/s00261-019-02236-4 [5] Rowe SP, Chu LC, Fishman EK. Initial experience with 3D CT cinematic rendering of acute pancreatitis and associated complications[J]. Abdom Radiol (NY), 2020, 45(5): 1290-8. doi: 10.1007/s00261-019-02310-x [6] 阮志兵, 焦俊, 瞿金环, 等. 胰头部肿块型慢性胰腺炎的CT误诊分析[J]. 临床放射学杂志, 2018, 37(9): 1505-9. https://www.cnki.com.cn/Article/CJFDTOTAL-LCFS201809025.htm [7] 杜奕奇, 陈其奎, 李宏宇, 等. 中国急性胰腺炎诊治指南(2019年, 沈阳) [J]. 临床肝胆病杂志, 2019, 35(12): 2706-11. https://www.cnki.com.cn/Article/CJFDTOTAL-LCGD201912016.htm [8] 王泽锋, 王海军, 张俊晶, 等. 自身免疫性胰腺炎CT及MRI影像学特征与诊断[J]. 中华消化外科杂志, 2017, 16(1): 95-101. doi: 10.3760/cma.j.issn.1673-9752.2017.01.018 [9] Srisajjakul S, Prapaisilp P, Bangchokdee S. CT and MR features that can help to differentiate between focal chronic pancreatitis and pancreatic cancer[J]. Radiol Med, 2020, 125(4): 356-64. doi: 10.1007/s11547-019-01132-7 [10] Arvanitakis M, Dumonceau JM, Albert J, et al. Endoscopic management of acute necrotizing pancreatitis: European society of gastrointestinal endoscopy (ESGE) evidence-based multidisci-plinary guidelines[J]. Endoscopy, 2018, 50(5): 524-46. doi: 10.1055/a-0588-5365 [11] Utrera Pérez E, Tárdaguila de la Fuente G, Martínez Rodríguez C, et al. Quantification of iodine concentration by dual-energy CT in patients with acute pancreatitis[J]. Radiologia, 2020, 62(5): 360-4. doi: 10.1016/j.rx.2019.12.007 [12] 杨丹丹, 林峤, 张小明. 新亚特兰大标准下急性坏死性胰腺炎的CT/ MRI评价[J]. 中国医学计算机成像杂志, 2018, 24(6): 495-9. doi: 10.3969/j.issn.1006-5741.2018.06.010 [13] 郭严, 陈东风, 孙文静. CT评估人体脂肪面积与急性高脂血症性胰腺炎复发的相关性研究[J]. 第三军医大学学报, 2019, 41(14): 1370-3. https://www.cnki.com.cn/Article/CJFDTOTAL-DSDX201914013.htm [14] 雍惠芳, 董雪, 王文森, 等. IgG4相关性胰腺炎CT和MRI检查的影像学特征[J]. 中华消化外科杂志, 2019, 18(7): 689-97. doi: 10.3760/cma.j.issn.1673-9752.2019.07.014 [15] 王雅杰, 崔文静, 陈晓, 等. 增强CT对乏血供胰腺神经内分泌肿瘤及肿块型胰腺炎的鉴别诊断价值[J]. 医学研究生学报, 2020, 33(7): 732-6. https://www.cnki.com.cn/Article/CJFDTOTAL-JLYB202007012.htm [16] 彭容, 张小明, 张凌, 等. 急性胰腺炎伴肺炎的CT表现及其与临床相关性分析[J]. 放射学实践, 2020, 35(1): 68-73. https://www.cnki.com.cn/Article/CJFDTOTAL-FSXS202001020.htm [17] French JM, Twedt DC, Rao S, et al. CT angiographic changes in dogs with acute pancreatitis: a prospective longitudinal study[J]. Vet Radiol Ultrasound, 2020, 61(1): 33-9. doi: 10.1111/vru.12816 [18] Martin SS, Trapp F, Wichmann JL, et al. Dual-energy CT in early acute pancreatitis: improved detection using iodine quantification[J]. Eur Radiol, 2019, 29(5): 2226-32. doi: 10.1007/s00330-018-5844-x [19] Park S, Chu LC, Hruban RH, et al. Differentiating autoimmune pancreatitis from pancreatic ductal adenocarcinoma with CT radiomics features[J]. Diagn Interv Imaging, 2020, 101(9): 555-64. doi: 10.1016/j.diii.2020.03.002 [20] 阮志兵, 焦俊, 闵定玉, 等. 急性胰腺炎胰腺内外病变的CT与MRI诊断价值[J]. 中华普通外科杂志, 2018, 33(9): 729-33. doi: 10.3760/cma.j.issn.1007-631X.2018.09.005 [21] Pereira M, Prakash A, Puranik AD, et al. Regorafenib-associated acute pancreatitis diagnosed on 18F-FDG PET/CT[J]. Clin Nucl Med, 2021, 46(5): e256-7. doi: 10.1097/RLU.0000000000003449 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 151
- HTML全文浏览量: 103
- PDF下载量: 1
- 被引次数: 0