



Comparison of imaging features between echocardiography and MSCT in emergency aortic dissection
-
摘要:
目的探讨经胸超声心动图(TTE)和多层螺旋CT(MSCT)在急诊主动脉夹层诊断中的应用价值。 方法选取2016年1月~2020年4月在我院治疗的疑似主动脉夹层患者141例,给予TTE和MSCT检查,分析两者诊断价值差异;分析主动脉夹层和非主动脉夹层MSCT征象差异,以及主动脉夹层不同分型MSCT征象差异。 结果141例疑似主动脉夹层患者,经手术或CT血管成像确诊112例主动脉夹层患者,29例为非主动脉夹层患者;MSCT诊断主动脉夹层的敏感度、准确性和阴性预测值分别为95.54%、94.33%和83.87%,明显高于TTE诊断(P < 0.05);MSCT和TTE诊断主动脉夹层的特异性和阳性预测值比较差异无统计学意义(P>0.05);MSCT征象中,主动脉夹层中钙化内移、主动脉区高密度、线样征和主动脉增宽的比例高于非主动脉夹层(P < 0.05);主动脉夹层和非主动脉夹层中心包积液、胸腔积液比例差异无统计学意义(P>0.05);MSCT征象中,A型主动夹层中主动脉区高密度比例高于B型主动脉夹层(P < 0.05);A型和B型主动脉夹层中钙化内移、线样征、心包积液、胸腔积液和主动脉增宽比例比较差异无统计学意义(P>0.05)。 结论相较于TTE,MSCT在急诊主动脉夹层诊断中有较好的应用价值,值得临床使用。 Abstract:ObjectiveTo evaluate the value of transthoracic echocardiography(TTE)and multi-slice spiral CT(MSCT)in thediagnosis of aortic dissection in emergency. MethodsA total of 141 patients with suspected aortic dissection who were treatedin our hospital from January 2016 to April 2020 were selected.The TTE and MSCT were examined, the difference of diagnosticvalue between them was analyzed by χ2 test, the differences of MSCT signs between aortic dissection and non-aortic dissection, as well as the differences of MSCT signs between different types of aortic dissection were analyzed. ResultsAmong 141suspected aortic dissection patients, 112 patients were diagnosed as aortic dissection by surgery or CT angiography, and 29patients were non aortic dissection patients.The sensitivity, accuracy and negative predictive values of MSCT in the diagnosisof aortic dissection were 95.54%, 94.33% and 83.87%, which were significantly higher than that of TTE(P < 0.05).There were nosignificant difference in specificity and positive predictive value between MSCT and TTE in the diagnosis of aortic dissection(P>0.05).Among the MSCT signs, the proportions of calcification metastasis, aortic area density, linear pattern and aorticwidening in aortic dissection were significantly higher than those in non-aortic dissection(P < 0.05).There was no significantdifference in the proportion of central effusion and pleural effusion between aortic dissection and non-aortic dissection(P>0.05).In MSCT findings, the high density ratio of aortic area in type A active aortic dissection was significantly higher than thatin type B active aortic dissection(P < 0.05).There was no significant difference in the proportion of calcification metastasis, linear sign, pericardial effusion, pleural effusion and aortic widening between type A and type B aortic dissection(P>0.05). ConclusionCompared with TTE, MSCT has better application value in the diagnosis of emergency aortic dissection and isworthy of clinical use. -

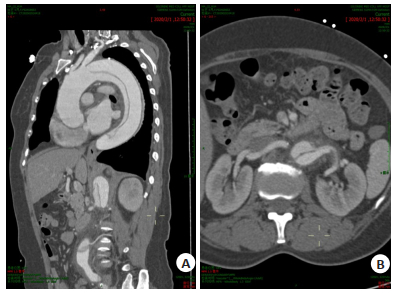
图 1 主动脉夹层A型
A: 可见升主动脉扩张; B: 真腔较窄, 假腔较宽; C: 下缘至双侧恰内外动脉
Figure 1. Aortic dissection type A.

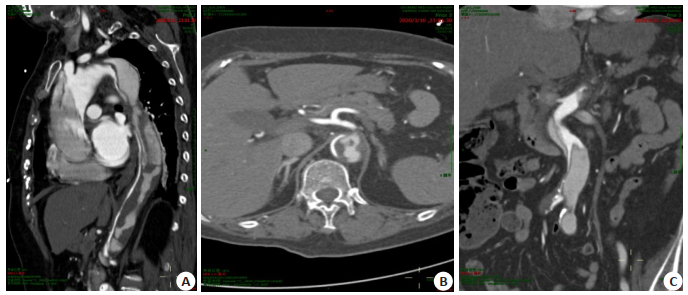
图 2 主动脉夹层B型
A: 主动脉弓以下管腔增粗; B: 腹主动脉周围多发渗出, 主动脉夹层累及左肾动脉
Figure 2. Aortic dissection type B.
表 1 主动脉夹层和非主动脉夹层患者一般资料比较
Table 1. Comparison of general data of patients with aortic dissection and patients without aortic dissection
组别 男/女 年龄(岁, Mean±SD) 高血压[n(%)] 糖尿病[n(%)] 主动脉夹层(n=112) 62/50 52.87±11.32 72(64.29) 35(31.25) 非主动脉夹层(n=29) 20/9 51.89±10.15 20(68.97) 8(27.59) t/χ2 1.753 0.424 0.222 0.146 P 0.186 0.672 0.637 0.703  下载: 导出CSV
下载: 导出CSV
表 2 TTE、MSCT诊断主动脉夹层价值比较
Table 2. Comparison of value of TTE and MSCT in the diagnosis of aortic dissection (%)
组别 敏感度 特异性 准确性 阳性预测值 阴性预测值 TTE 72.32(81/112) 93.10(27/29) 77.31(109/141) 97.59(81/83) 46.55(27/58) MSCT 95.54(107/112) 89.66(26/29) 94.33(133/141) 97.27(107/110) 83.87(26/31) χ2 22.374 0.000 16.780 0.000 11.681 P 0.000 1.000 0.000 1.000 0.001
下载: 导出CSV
表 3 主动脉夹层和非主动脉夹层MSCT征象比较
Table 3. Comparison of MSCT signs between aortic dissection and non-aortic dissection[n(%)]
组别 钙化内移 主动脉区高密度 线样征 心包积液 胸腔积液 主动脉增宽 主动脉夹层(n=112) 72(64.29) 49(43.75) 81(72.32) 5(4.46) 26(23.21) 82(73.21) 非主动脉夹层(n=29) 3(10.34) 0(0.00) 2(6.90) 1(3.45) 6(20.69) 7(24.14) χ2 26.919 19.445 40.721 0.000 0.084 23.833 P 0.000 0.000 0.000 1.000 0.772 0.000
下载: 导出CSV
表 4 主动脉夹层不同分型MSCT征象比较
Table 4. Comparison of MSCT signs of different types of aortic dissection[n(%)]
组别 钙化内移 主动脉区高密度 线样征 心包积液 胸腔积液 主动脉增宽 A型(n=35) 24(68.75) 28(80.00) 25(71.43) 2(5.71) 9(25.71) 27(77.14) B型(n=77) 48(62.33) 21(27.27) 56(72.73) 3(3.90) 17(22.08) 55(71.43) χ2 0.407 27.184 0.020 0.000 0.179 0.401 P 0.523 0.000 0.887 1.000 0.673 0.527
下载: 导出CSV
-
[1] Ibrahim I, Chua MT, Tan DW, et al. Impact of 24-hour specialist coverage and an on-site CT scanner on the timely diagnosis of acute aortic dissection[J]. Singap Med J, 2020, 61(2): 86-91. doi: 10.11622/smedj.2019039 [2] Orabi NA, Quint LE, Watcharotone K, et al. Distinguishing acute from chronic aortic dissections using CT imaging features[J]. Int J Cardiovasc Imaging, 2018, 34(11): 1831-40. doi: 10.1007/s10554-018-1398-x [3] Harris RJ, Kim S, Lohr J, et al. Classification of aortic dissection and rupture on post-contrast CT images using a convolutional neural network[J]. J Digit Imaging, 2019, 32(6): 939-46. doi: 10.1007/s10278-019-00281-5 [4] Patel VK, Fruauff A, Esses D, et al. Implementation of an aortic dissection CT protocol with clinical decision support aimed at decreasing radiation exposure by reducing routine abdominopelvic imaging[J]. Clin Imaging, 2020, 67: 108-12. doi: 10.1016/j.clinimag.2020.06.005 [5] Masri A, Bianco V, Kilic A, et al. Failure of CT angiogram to detect an ascending aortic dissection[J]. J Card Surg, 2018, 33(4): 194-5. doi: 10.1111/jocs.13562 [6] Hofmeister S, Thomas MB, Paulisin J, et al. Endovascular management of ruptured abdominal aortic aneurysms and acute aortic dissections [J]. Vasa, 2019, 48(1): 35-46. doi: 10.1024/0301-1526/a000760 [7] Mark DG, Davis JA, Hung YY, et al. Discriminatory value of the ascending aorta diameter in suspected acute type A aortic dissection [J]. Acad Emerg Med, 2019, 26(2): 217-25. doi: 10.1111/acem.13547/abstract [8] 阮仕波, 阮世文. 对比分析急诊主动脉夹层应用多层螺旋CT和超声心动图诊断的应用价值[J]. 现代医用影像学, 2019, 28(11): 2415-7. https://www.cnki.com.cn/Article/CJFDTOTAL-XDYY201911021.htm [9] Hahn LD, Mistelbauer G, Higashigaito K, et al. CT-based true- and false-lumen segmentation in type B aortic dissection using machine learning[J]. Radiol: Cardiothorac Imaging, 2020, 2(3): e190179. doi: 10.1148/ryct.2020190179 [10] 陈炯, 何飞. 64层螺旋CT对主动脉夹层真假腔的鉴别诊断再探讨[J]. 中国CT和MRI杂志, 2018, 16(1): 79-81. https://www.cnki.com.cn/Article/CJFDTOTAL-CTMR201801025.htm [11] 罗常有, 王善花, 陈本发, 等. 急性主动脉夹层168例临床诊治分析[J]. 临床误诊误治, 2018, 31(2): 1-5. https://www.cnki.com.cn/Article/CJFDTOTAL-LCWZ201802002.htm [12] Hwang SO, Cha KC. Diagnosis of aortic dissection during cardiopulmonary resuscitation. Transthoracic versus transesophageal echocardiography[J]. Am J Emerg Med, 2020, 38(4): 829-30. doi: 10.1016/j.ajem.2020.02.014 [13] 任陇滨. MSCT与超声心动图在急诊疑似主动脉夹层患者中的应用[J]. 中国CT和MRI杂志, 2019, 17(4): 68-71. https://www.cnki.com.cn/Article/CJFDTOTAL-CTMR201904022.htm [14] 王建, 刘何鹏. 多层螺旋CT诊断主动脉夹层临床分析[J]. 医学影像学杂志, 2018, 28(6): 929-32. https://www.cnki.com.cn/Article/CJFDTOTAL-XYXZ201806016.htm [15] 陈明江, 姜建彪, 李梅. 多层螺旋CT血管造影表现对主动脉夹层患者院内生存状况的影响[J]. 中国现代医学杂志, 2019, 29(10): 105-8. https://www.cnki.com.cn/Article/CJFDTOTAL-ZXDY201910022.htm [16] 路洪剑, 刘莹, 唐栋. 复杂急性主动脉综合征的多层螺旋CT血管成像研究及价值探讨[J]. 中西医结合心脑血管病杂志, 2018, 16(13): 1898-900. doi: 10.12102/j.issn.1672-1349.2018.13.035 [17] 徐军明, 张本贵, 马渝. 多普勒超声和MSCTA诊断主动脉夹层的价值分析[J]. 中国CT和MRI杂志, 2020, 18(1): 51-3, 78. https://www.cnki.com.cn/Article/CJFDTOTAL-CTMR202001017.htm [18] Allen BD, Aouad PJ, Burris NS, et al. Detection and hemodynamic evaluation of flap fenestrations in type B aortic dissection with 4D flow MRI: comparison with conventional MRI and CT angiography [J]. Radiol: Cardiothorac Imaging, 2019, 1(1): e180009. http://www.onacademic.com/detail/journal_1000042303911799_77fd.html [19] 王正, 左玉强, 王晓彤, 等. 原发性肺黏膜相关淋巴组织淋巴瘤临床及MDCT影像表现分析[J]. 国际呼吸杂志, 2020, 40(13): 1017-21. [20] 郭卫红, 黄晓云, 王雪伟, 等. MSCT与超声心动图在急诊主动脉夹层患者诊断准确率中的比较[J]. 中国CT和MRI杂志, 2020, 18(4): 60-3. https://www.cnki.com.cn/Article/CJFDTOTAL-CTMR202004019.htm [21] 欧阳永, 陈焕群, 崔冰, 等. 64排128层螺旋CT血管成像检测主动脉夹层[J]. 分子影像学杂志, 2018, 41(1): 6-10. doi: 10.3969/j.issn.1674-4500.2018.01.02 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 331
- HTML全文浏览量: 140
- PDF下载量: 3
- 被引次数: 0