



Value of ultrasound combined with thoracoscopy in the diagnosis of benign and malignant pleural effusion
-
摘要:
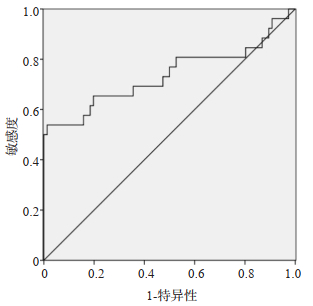
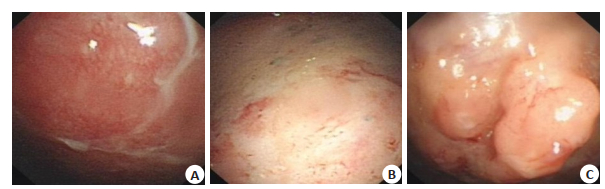
目的探讨超声联合胸腔镜在胸腔积液良恶性诊断中的价值。 方法选取2020年1月~2021年3月在我院就诊的不明原因的胸腔积液患者102例,其中,良性患者76例,恶性患者26例,分析良恶性胸腔积液患者胸腔镜下形态、超声特征差异。分析胸膜厚度鉴别良恶性胸腔积液的价值和超声联合胸腔镜诊断良恶性胸腔积液的价值。 结果良性患者病因均为结核性胸膜炎,恶性患者病因以胸膜转移性腺癌为主(88.46%);恶性组胸腔镜下胸膜肿块、胸膜瓷片状增厚的比例高于良性组(P < 0.05),而胸膜充血水肿、胸膜粘连带比例分低于良性组(P < 0.05);恶性组胸膜厚度、胸膜非均匀性增厚比例明显高于良性组(P < 0.05),而强回声纤维分隔带比例低于良性组(P < 0.05);胸膜厚度鉴别恶性胸腔积液的ROC曲线下面积为0.736(P < 0.05),截断值为10.73mm,敏感度和特异性分别为53.80%和99.70%;超声联合胸腔镜下形态诊断恶性胸腔积液的敏感度、特异性、准确率、阳性预测值和阴性预测值分别为76.92%、81.58%、80.39%、58.82%和91.18%。 结论超声联合胸腔镜在胸腔积液良恶性诊断中有一定的应用价值。 Abstract:ObjectiveTo explore the value of ultrasound combined with thoracoscopy in the diagnosis of benign and malignantpleural effusion. MethodsA total of 102 patients with unexplained pleural effusion in our hospital from January 2020 to March2021 were selected.The differences of thoracoscopic morphology and ultrasound characteristics between benign andmalignant pleural effusion patients were analyzed. ResultsIn the 102 patients, 76 were benign and 26 were malignant.Theetiology of benign patients was tuberculous pleurisy, while the main cause of malignant was metastatic adenocarcinoma ofpleura, accounting for 88.46%.The proportions of pleural mass and porcelain like thickening in malignant group were higherthan those in benign group(P < 0.05).The proportions of pleural congestion and edema and pleural adhesions were lower thanthose in benign group(P < 0.05).In the malignant group, the pleural thickness and the proportion of non-uniform pleuralthickening were significantly higher than those in benign group(P < 0.05).The proportion of hyperechoic fiber septum wassignificantly lower than that in benign group(P < 0.05).The area under the ROC curve of membrane thickness in differentiatingmalignant pleural effusion was 0.736(P < 0.05), and the cut-off value was 10.73 mm, the sensitivity and specificity were 53.80%and 99.70%, respectively.The sensitivity, specificity, accuracy, positive predictive value and negative predictive value ofultrasonography combined with thoracoscopic morphological diagnosis of malignant pleural effusion were 76.92%, 81.58%, 80.39%, 58.82% and 91.18%, respectively. ConclusionUltrasound combined with thoracoscopy has a certain value in thediagnosis of benign and malignant pleural effusion. -
Key words:
- ultrasound /
- thoracoscopy /
- pleural effusion /
- benign and malignant /
- diagnostic value
-
表 1 良性和恶性患者临床一般资料比较
Table 1. Comparison of clinical data of benign and malignant patients [n(%)]
临床资料 良性组(n=76) 恶性组(n=26) t/χ2 P 性别 0.200 0.655 男 40(52.63) 15(57.69) 女 36(47.37) 11(42.31) 年龄(岁, Mean±SD) 57.89±12.03 59.03±11.16 -0.425 0.672 BM(I kg/m2, Mean±SD) 22.15±2.60 22.02±2.92 0.213 0.832 部位 0.000 1.000 单侧 69(90.79) 23(88.46) 双侧 7(9.21) 3(11.54) 胸腔积液量(mL) 0.221 0.895 < 500 44(57.89) 15(57.69) 500~800 28(36.84) 9(34.62) > 800 mL 4(5.26) 2(7.69)  下载: 导出CSV
下载: 导出CSV
表 2 良恶性胸腔积液胸腔镜下形态比较
Table 2. Comparison of benign and malignant pleural effusion under thorac oscope[n(%)]
镜下表现 良性组(n=76) 恶性组(n=26) χ2 P 胸膜充血水肿 32(42.11) 3(11.54) 8.031 0.005 胸膜结节 29(38.16) 15(57.69) 3.014 0.083 胸膜肿块 3(3.95) 9(34.62) 14.722 0.000 胸膜粘连带 34(44.74) 5(19.23) 5.133 0.023 胸膜瓷片状增厚 3(3.95) 6(23.08) 6.595 0.010
下载: 导出CSV
表 3 良恶性胸腔积液超声特征比较
Table 3. Comparison of ultrasound features between benign and malignant pleural effusions
镜下表现 良性组(n=76) 恶性组(n=26) t/χ2 P 胸膜厚度(mm, Mean±SD) 8.72±1.15 11.02±2.00 -7.173 0.000 胸膜非均匀性增厚[n(%)] 11(14.47) 23(88.46) 47.722 0.000 强回声纤维分隔带[n(%)] 60(78.95) 5(19.23) 29.886 0.000
下载: 导出CSV
-
[1] Benlloch S, Galbis-Caravajal JM, Martín C, et al. Potential diagnostic value of methylation profile in pleural fluid and serum from cancer patients with pleural effusion[J]. Cancer, 2006, 107(8): 1859-65. doi: 10.1002/cncr.22190 [2] 刘文媛, 刘跃建, 高凌云. 良恶性胸腔积液的病因及不同诊断方法的研究进展[J]. 实用医院临床杂志, 2019, 16(1): 216-8. doi: 10.3969/j.issn.1672-6170.2019.01.069 [3] 樊英, 李龙芸. 良恶性胸腔积液的鉴别诊断[J]. 癌症进展, 2005, 3 (2): 134-8, 105. doi: 10.3969/j.issn.1672-1535.2005.02.012 [4] 陈聪, 李再清, 刘卫庭. 肿瘤标志物在恶性胸水中的诊断价值探讨[J]. 医药前沿, 2019, 9(5): 26-8. doi: 10.3969/j.issn.2095-1752.2019.05.014 [5] 刘岩, 刘勇, 孙如坤, 等. 内科胸腔镜对不同病因胸腔积液的鉴别诊断价值[J]. 中国实用医刊, 2021, 48(6): 23-6. doi: 10.3760/cma.j.cn115689-20201128-05827 [6] 李琚, 项尖尖, 王宝华, 等. 超声检查胸膜增厚对胸腔积液良恶性鉴别诊断的意义[J]. 影像研究与医学应用, 2019, 3(22): 209-10. https://www.cnki.com.cn/Article/CJFDTOTAL-YXYY201922138.htm [7] 李玉林. 病理学[M]. 北京: 人民卫生出版社, 2006. [8] Topalak O, Saygili U, de Soyturk M, et al. Serum, pleural effusion, and ascites CA-125 levels in ovarian cancer and nonovarian benign and malignant diseases: a comparative study[J]. Gynecol Oncol, 2002, 85(1): 108-13. doi: 10.1006/gyno.2001.6575 [9] Allama AM, Abou-Elela DH, Ibrahim IM. Pleural and serum markers for diagnosis of malignant pleural effusion[J]. Asian Cardiovasc Thorac Ann, 2020, 28(9): 560-5. doi: 10.1177/0218492320948311 [10] Dongel I, Gokmen A, Camas H, et al. Diagnostic significance of biochemical markers and pentraxin-3 in the differential diagnosis of malign, benign pleural effusion and empyema[J]. J Pak Med Assoc, 2020: 1. http://www.ncbi.nlm.nih.gov/pubmed/32400742 [11] Bao Q, Xu Y, Ding M, et al. Identification of differentially expressed miRNAs in differentiating benign from malignant pleural effusion [J]. Hereditas, 2020, 157(1): 6. doi: 10.1186/s41065-020-00119-z [12] Basso SMM, Lumachi F, Del Conte A, et al. Diagnosis of malignant pleural effusion using CT scan and pleural-fluid cytology together. A preliminary case-control study[J]. Anticancer Res, 2020, 40(2): 1135-9. doi: 10.21873/anticanres.14054 [13] Mohammed OM, Hussein KM, Ramadan AE, et al. Diagnostic value of calprotectin in differentiation between benign and malignant pleural effusion[J]. Egypt J Bronchol, 2019, 13(3): 382-7. doi: 10.4103/ejb.ejb_77_18 [14] Beheshtirouy S, Kakaei F, Mirzaaghazadeh M. Video assisted rigid thoracoscopy in the diagnosis of unexplained exudative pleural effusion[J]. J Cardiovasc Thorac Res, 2013, 5(3): 87-90. http://www.ncbi.nlm.nih.gov/pubmed/24252982 [15] Anavlavis S, Kouliatsis G, Sotiriou I, et al. AB 91. Prognostic factors in patients with malignant pleural effusion who underwent thoracoscopy diagnostic[J]. J Thoracic Dis, 2012, 4(1): 1163-4. http://europepmc.org/articles/PMC3537439 [16] Ram Kumar Gupta G, Raghavendra C, Roopa A, et al. Diagnostic efficacy of thoracoscopy in recurrent undiagnosed pleural effusion [J]. IP Indian J Immunol Respir Med, 2019, 4(2): 94-7. doi: 10.18231/j.ijirm.2019.022 [17] Bhatnagar R, Luengo-Fernandez R, Kahan BC, et al. Thoracoscopy and talc poudrage compared with intercostal drainage and talc slurry infusion to manage malignant pleural effusion: the TAPPS RCT[J]. Heal Technol Assess Winch Engl, 2020, 24(26): 1-90. doi: 10.3310/hta24260 [18] Ferrer J, Roldán J, Teixidor J, et al. Predictors of pleural malignancy in patients with pleural effusion undergoing thoracoscopy[J]. Chest, 2005, 127(3): 1017-22. doi: 10.1378/chest.127.3.1017 [19] 蓝思荣, 李雄, 许建辉. 高频超声引导下胸膜活检对渗出性胸腔积液诊断价值[J]. 现代医用影像学, 2020, 29(3): 558-9, 562. https://www.cnki.com.cn/Article/CJFDTOTAL-XDYY202003056.htm [20] 时绍奖. 恶性胸膜病变25例超声分析[J]. 内科, 2009, 4(3): 361-2. doi: 10.3969/j.issn.1673-7768.2009.03.013 [21] Qureshi NR, Rahman NM, Gleeson FV. Thoracic ultrasound in the diagnosis of malignant pleural effusion[J]. Thorax, 2009, 64(2): 139-43. doi: 10.1136/thx.2008.100545 -

 点击查看大图
点击查看大图
图(2) / 表(3)
计量
- 文章访问数: 319
- HTML全文浏览量: 112
- PDF下载量: 2
- 被引次数: 0