



Clinical diagnostic value of MDCT in angiomyolipomas with minimal fat
-
摘要:
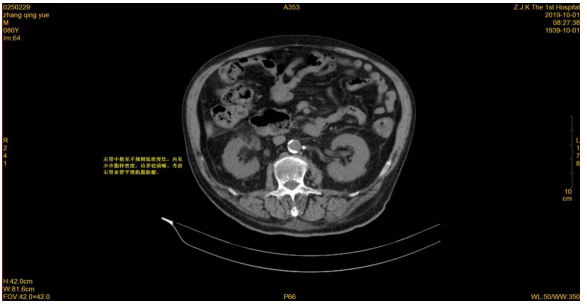
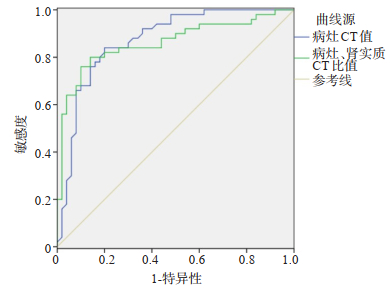
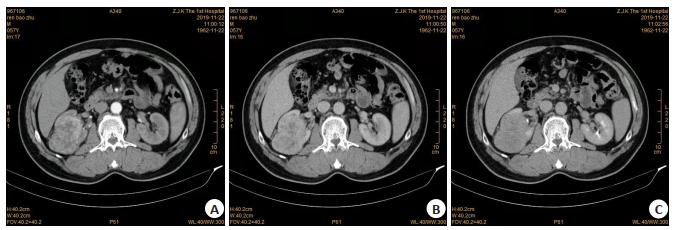
目的探讨多排螺旋CT(MDCT)在乏脂性肾血管平滑肌脂肪瘤诊断中的应用价值。 方法选取2012年1月~2020年2月在我院治疗的乏脂性肾血管平滑肌脂肪瘤患者作为观察组(n=117),将肾透明细胞癌患者作为对照组(n=210),两组均给予MDCT检查,分析两组CT征象、CT值等差异,采用受试者工作特征(ROC)曲线分析CT值判断乏脂性肾血管平滑肌脂肪瘤的价值。 结果观察组女性比例高于对照组(P < 0.05),年龄低于对照组(P < 0.05);观察组密度均匀、边界清楚、瘤内血管影比例分别为80.34%、100.00%和16.24%,明显高于对照组(P < 0.05);观察组假包膜比例低于对照组(P < 0.05);CT征象中,形态、强化方式在观察组和对照组中差异无统计学意义(P>0.05);观察组病灶CT值和病灶/肾实质CT比值分别为46.10±7.82 Hu和1.37±0.32,明显高于对照组(P < 0.05);观察组和对照组肾实质CT值比较差异无统计学意义(P>0.05);病灶CT值、病灶/肾实质CT比值诊断乏脂性肾血管平滑肌脂肪瘤的ROC曲线下面积分别为0.872和0.862,截断值分别为41.50 Hu和1.20时,敏感度分别为78.80%和76.50%,特异性分别为75.50%和74.40%。 结论MDCT在乏脂性肾血管平滑肌脂肪瘤诊断中有较好的应用价值,值得临床使用。 -
关键词:
- 多排螺旋CT /
- 乏脂性肾血管平滑肌脂肪瘤 /
- 肾透明细胞癌 /
- 诊断价值
Abstract:ObjectiveTo evaluate the value of multidetector CT(MDCT)in the diagnosis of angiomyolipomas with minimal fat. MethodsA total of 117 patients with angiomyolipomas with minimal fat who were treated in our hospital from January 2012to February 2020 were selected as the observation group, 210 patients with renal clear cell carcinoma were control group.Bothgroups were given MDCT examination.The differences of CT signs and CT values between the two groups were analyzed.The receiver operating characteristic(ROC)curve was used to analyze the CT value in the diagnosis of angiomyolipomas withminimal fat. ResultsThe female proportion of the observation group was higher than that of the control group(P < 0.05).Theage of the observation group was lower than that of the control group(P < 0.05).In the observation group, the proportion of thedensity was uniform, the boundary was clear, and vascular shadow in the tumor were 80.34%, 100.00% and 16.24%, whichwere significantly higher than that in the control group(P < 0.05).The proportion of pseudocapsule in the observation groupwas significantly lower than that in the control group(P < 0.05).In CT signs, there were no significant difference in morphologyand enhancement mode between the observation group and the control group(P>0.05).The lesion CT value and CT ratio oflesion/renal parenchyma in the observation group were 46.10±7.82 Hu and 1.37±0.32, which were significantly higher thanthose in the control group(P < 0.05).There was no significant difference in CT value of renal parenchyma between theobservation group and the control group(P>0.05).The area under ROC curve of lesion CT value and lesion/renal parenchymaCT ratio in the diagnosis of angiomyolipomas with minimal fat were 0.872 and 0.862, cut-off values were 41.50 Hu and 1.20, the sensitivity were 78.80% and 76.50%, and the specificity were 75.50% and 74.40%. ConclusionMDCT has a good value inthe diagnosis of angiomyolipomas with minimal fat, which is worthy of clinical use. -
表 1 观察组和对照组一般资料比较
Table 1. Comparison of general data between observation group and control group
组别 男/女(n) 年龄(Mean±SD,岁) BM(I Mean±SD,kg/m2) 高血压[n(%)] 糖尿病[n(%)] 观察组(n=117) 38/79 50.12±12.03 22.10±2.03 54(46.15) 30(25.64) 对照组(n=210) 132/78 57.80±11.13 22.16±2.01 103(49.05) 51(24.29) t/χ2 27.780 -5.809 -0.258 0.252 0.074 P 0.000 0.000 0.797 0.616 0.786  下载: 导出CSV
下载: 导出CSV
表 2 观察组和对照组CT征象比较
Table 2. Comparison of CT signs between observation group and control group[n(%)]
CT征象 观察组(n=117) 对照组(n=210) χ2 P 形态 0.015 0.902 规则 81(69.23) 144(68.57) 不规则 36(30.77) 66(31.43) 密度 106.710 0.000 均匀 94(80.34) 45(21.43) 不均匀 23(19.66) 165(78.57) 边界 17.729 0.000 清楚 117(100.00) 181(86.19) 不清楚 0(0.00) 29(13.81) 假包膜 113.905 0.000 有 4(3.42) 135(64.29) 无 113(96.58) 75(35.71) 瘤内血管影 5.087 0.024 有 19(16.24) 17(8.10) 无 98(83.76) 193(91.9) 强化方式 2.653 0.265 快进快出 51(43.59) 98(46.67) 持续强化 62(52.99) 110(52.38) 延迟强化 4(3.42) 2(0.95)
下载: 导出CSV
表 3 观察组和对照组病灶CT值比较
Table 3. Comparison of CT values of lesions between observation group and control group (Mean±SD)
组别 病灶CT值(Hu) 肾实质CT值(Hu) 病灶/肾实质CT比值 观察组(n=117) 46.10±7.82 33.72±4.80 1.37±0.32 对照组(n=210) 31.12±7.22 32.55±6.92 0.95±0.21 t 17.454 1.624 14.290 P 0.000 0.105 0.000
下载: 导出CSV
-
[1] Idogawa M, Hida T, Tanaka T, et al. Renal angiomyolipoma (AML) harboring a missense mutation of TSC2 with copy-neutral loss of heterozygosity (CN-LOH)[J]. Cancer Biol Ther, 2020, 21(4): 315-9. doi: 10.1080/15384047.2019.1702406 [2] Wang C, Li X, Peng L, et al. An update on recent developments in rupture of renal angiomyolipoma[J]. Medicine: Baltimore, 2018, 97 (16): e0497. doi: 10.1097/MD.0000000000010497 [3] Lim RS, Flood TA, McInnes MDF, et al. Renal angiomyolipoma without visible fat: Can we make the diagnosis using CT and MRI? [J]. Eur Radiol, 2018, 28(2): 542-53. doi: 10.1007/s00330-017-4988-4 [4] Nie P, Yang GJ, Wang ZG, et al. A CT-based radiomics nomogram for differentiation of renal angiomyolipoma without visible fat from homogeneous clear cell renal cell carcinoma[J]. Eur Radiol, 2020, 30(2): 1274-84. doi: 10.1007/s00330-019-06427-x [5] You MW, Kim N, Choi HJ. The value of quantitative CT texture analysis in differentiation of angiomyolipoma without visible fat from clear cell renal cell carcinoma on four-phase contrastenhanced CT images[J]. Clin Radiol, 2019, 74(7): 547-54. doi: 10.1016/j.crad.2019.02.018 [6] Siegel C. Re: diagnostic performance of CT for diagnosis of fat-poor angiomyolipoma in patients with renal masses: a systematic review and meta-analysis[J]. J Urol, 2018, 199(6): 1376. http://europepmc.org/abstract/MED/29783555 [7] Liu X, Ma X, Liu Q, et al. Retroperitoneal laparoscopic nephron sparing surgery for large renal angiomyolipoma: Our technique and experience. A case series of 41 patients[J]. Int J Surg, 2018, 54(pt a): 216-21. http://www.ncbi.nlm.nih.gov/pubmed/29723675 [8] Swärd J, Henrikson O, Lyrdal D, et al. Renal angiomyolipomapatient characteristics and treatment with focus on active surveillance[J]. Scand J Urol, 2020, 54(2): 141-6. doi: 10.1080/21681805.2020.1716066 [9] Inoue C, Saito R, Nakanishi W, et al. Renal epithelioid angiomyolipoma undergoing aggressive clinical outcome: the MDM2 expression in tumor cells of two cases[J]. Tohoku J Exp Med, 2019, 247(2): 119-27. doi: 10.1620/tjem.247.119 [10] 王思凯, 李鸣瑶, 梁卡丽, 等. 多排螺旋CT诊断乏脂性肾血管平滑肌脂肪瘤与肾癌的对照研究[J]. 中国医学计算机成像杂志, 2018, 24(3): 215-8. https://www.cnki.com.cn/Article/CJFDTOTAL-YJTY201803007.htm [11] 丁玉芹, 于泳, 罗荣奎, 等. 多元logistic回归分析CT征象鉴别乏脂肪血管平滑肌脂肪瘤和肾透明细胞癌的价值[J]. 临床放射学杂志, 2019, 38(3): 495-9. https://www.cnki.com.cn/Article/CJFDTOTAL-LCFS201903032.htm [12] 李珂, 李彦锋, 江军, 等. 增强CT扫描可鉴别诊断少见肾细胞癌亚型[J]. 分子影像学杂志, 2020, 43(3): 415-21. doi: 10.12122/j.issn.1674-4500.2020.03.10 [13] Francesca B, Giulia C, Luisella R, et al. Human renal angiomyolipoma cells of male and female origin can migrate and are influenced by microenvironmental factors[J]. Plos One, 2018, 13(6): e0199371. doi: 10.1371/journal.pone.0199371 [14] Barnett JR, Grinspoon RA, Harisinghani M, et al. The efficacy of cannabidiol on renal angiomyolipoma and subependymal giant cell tumor volume in tuberous sclerosis complex[J]. J Clin Neurosci, 2020, 77: 85-8. doi: 10.1016/j.jocn.2020.05.030 [15] 丁冠融, 李涵默, 庄君龙. 多排螺旋CT检查对乏脂肪肾血管平滑肌脂肪瘤的诊断价值[J]. 实用癌症杂志, 2019, 34(7): 1201-3, 1207. doi: 10.3969/j.issn.1001-5930.2019.07.045 [16] 姜国锦, 方松华. MSCT对肾上皮样血管平滑肌脂肪瘤与肾透明细胞癌的鉴别诊断价值[J]. 医学影像学杂志, 2018, 28(8): 1322-5. https://www.cnki.com.cn/Article/CJFDTOTAL-XYXZ201808029.htm [17] 马光明, 呼延静, 曹媛, 等. 能谱CT鉴别肾透明细胞癌和乏脂型肾血管平滑肌脂肪瘤的应用[J]. 影像诊断与介入放射学, 2018, 27(4): 278-82. https://www.cnki.com.cn/Article/CJFDTOTAL-YXZD201804006.htm [18] 徐贝, 孙浩然, 张泽伟. 乏脂肾血管平滑肌脂肪瘤与非透明细胞肾癌的CT鉴别诊断[J]. 中国医学影像学杂志, 2018, 26(6): 431-7. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYYZ201806008.htm [19] 张丽青, 韩志江. 最大径≤3 cm的乏脂肪肾脏血管平滑肌脂肪瘤与肾透明细胞癌的MRI鉴别[J]. 临床放射学杂志, 2019, 38(1): 132-5. https://www.cnki.com.cn/Article/CJFDTOTAL-LCFS201901031.htm [20] 高原, 蔡晓娟, 陆建东. 增强CT鉴别诊断乏脂性肾血管平滑肌脂肪瘤与肾癌的影像特征及临床价值[J]. 癌症进展, 2018, 16 (10): 1231-3, 1237. https://www.cnki.com.cn/Article/CJFDTOTAL-AZJZ201810010.htm -

 点击查看大图
点击查看大图
图(3) / 表(3)
计量
- 文章访问数: 327
- HTML全文浏览量: 178
- PDF下载量: 3
- 被引次数: 0