



Application value of ultrasound- guided low-temperature plasma technology in the surgical diagnosis and treatment of tonsillar hypertrophic snoring and dual sleep apnea syndrome
-
摘要:
目的探讨超声引导下低温等离子技术治疗扁桃体肥大引起儿童阻塞性睡眠呼吸暂停低通气综合征(OSAHS)中的效果。 方法选取淮南新华医疗集团新华医院收治的120例扁桃体肥大引起OSAHS患儿接受超声引导下低温等离子手术治疗,其中60例接受扁桃体全切作为全切组,60例接受扁桃体部分切除患儿作为非全切组,对比两组的手术时间、出血情况,患儿手术前后免疫功能、生活质量、睡眠监测指数的变化。 结果全切组的手术时间、出血量大于非全切组(P < 0.05);术前,全切组和非全切组外周血的CD3+、CD4+、CD8+、CD4+/CD8+差异无统计学意义(P>0.05);术后1月,非全切组的外周血的CD3+、CD4+、CD4+/CD8+测定值大于全切组(P < 0.05);术前及术后1月,全切组和非全切组睡眠紊乱、身体症状、情绪影响、白天问题、看护者关心评分差异无统计学意义(P>0.05);术后1月,两组患者的睡眠紊乱、身体症状、情绪影响、白天问题、看护者关心评分较本组术前均显著降低(P < 0.05);术前及术后1月,全切组和非全切组呼吸暂停低通气指数、最低血氧饱和度、平均血氧饱和度差异无统计学意义(P>0.05);术后1月,两组患者的呼吸暂停低通气指数较本组术前均降低(P < 0.05),最低血氧饱和度、平均血氧饱和度较本组术前均增高(P < 0.05)。 结论超声引导下低温等离子技术实施扁桃体部分切除与扁桃体全切的效果差异不大,但是前者具有手术时间短、创伤小,术后患儿免疫功能受到的影响更小的优势。 -
关键词:
- 低温等离子 /
- 扁桃体肥大 /
- 阻塞性睡眠呼吸暂停低通气综合征 /
- 免疫功能
Abstract:ObjectiveTo explore the effect of ultrasound-guided low-temperature plasma technology in the treatment of tonsil hypertrophy in children with obstructive sleep apnea-hypopnea syndrome (OSAHS). MethodsA total of 120 children with OSAHS caused by tonsillar hypertrophy were selected in Xinhua Hospital of Huainan Xinhua Medical Group to receive ultrasound-guided low-temperature plasma surgery. The 60 cases received total tonsillectomy (totalectomy group) and other 60 cases received partial tonsillectomy as non-totalectomy group. The operation time, bleeding, the immune function, quality of life, and sleep monitoring index of the children before and after the operation in the two groups were compared. ResultsThe operation time and blood loss of the total resection group were greater than those of the non-total resection group(P < 0.05). Before surgery, the difference of peripheral blood CD3+, CD4+, CD8+, CD4+/CD8+ between the total resection group and the non-total resection group was not significant (P>0.05). One month after operation, the peripheral blood CD3+, CD4+, CD4+/ CD8+ values of the non-total resection group were greater than those of the total resection group (P < 0.05). Before and 1 month after the operation, there was no significant difference in sleep disturbance, physical symptoms, emotional effects, daytime problems, and caregiver care scores between the total resection group and the non-full resection group (P>0.05). One month after the operation, the sleep disturbance, physical symptoms, emotional impact, daytime problems, and caregiver care scores of the patients in the group were significantly lower than those in the preoperative group (P < 0.05). Before and 1 month after the operation, there was no significant difference of AHI, minimum blood oxygen saturation, and average blood oxygen saturation between the total and non-total resection group (P>0.05). One month after surgery, the AHI of the two groups of patients were significantly lower than that of the preoperative group (P < 0.05). The blood oxygen saturation and average blood oxygen saturation were significantly higher than those of this group before operation (P < 0.05). ConclusionUltrasound-guided low-temperature plasma technology has little difference in effect between partial tonsillectomy and total tonsillectomy, but the former has the advantages of short operation time, less trauma, and less impact on the immune function of children after surgery. -
Key words:
- low temperature coblation /
- hypertrophy of tonsil /
- OSAHS /
- immunologic function
-

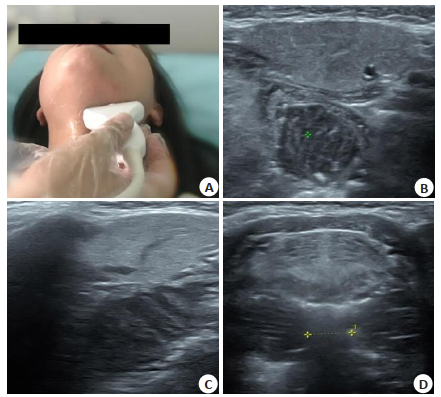
图 1 10岁女童,经超声检查诊断为扁桃体肥大Ⅲ度
A:女童接受术前超声检查;B:超声测量扁桃体的横径和前后径;C:测量患者扁桃体纵向最大横径;D:超声测量两扁桃体内径之间的距离.
Figure 1. A 10-year-old female patient, was diagnosed with tonsillar hypertrophy grade Ⅲ by ultrasound.
表 1 两组患儿的基线资料分析
Table 1. Baseline data analysis of the two groups of children(n=60, Mean±SD)
资料 全切组 非全切组 t/χ2 P 年龄(岁) 7.2±2.0 7.0±1.8 0.576 0.566 病程(年) 18.8±4.4 19.2±4.8 -0.476 0.635 身高(cm) 130.5±4.7 129.8±5.0 0.790 0.431 体质量(kg) 29.8±2.7 29.5±3.0 0.576 0.566 心率(次/min) 91.0±7.1 89.9±6.8 0.867 0.388 术前AHI(次/h) 14.2±2.6 13.9±3.2 0.564 0.574 性别[n(%)] 1.319 0.251 男 36(60.00) 42(70.00) 女 24(40.00) 18(30.00) 扁桃体肥大程度[n(%)] 1.976 0.160 Ⅱ度 21(35.00) 14(23.33) Ⅲ度 39(65.00) 46(76.67) AHI:呼吸暂停低通气指数  下载: 导出CSV
下载: 导出CSV
表 2 两组患儿手术时间、出血情况比较
Table 2. Comparison of operation time and bleeding betweenthe two groups of children(n=60, Mean±SD)
组别 手术时间(min) 出血情况(mL) 全切组 34.8±3.7 14.7±3.0 非全切组 29.7±4.0 12.5±2.8 t 7.250 4.153 P 0.000 0.000
下载: 导出CSV
表 3 两组患儿外周血T淋巴细胞比较
Table 3. Comparison of T lymphocytes in peripheral blood of two groups of children(n=60, Mean±SD)
因素 全切组 非全切组 t P CD3+(%) 术前 65.3±5.0 64.1±4.8 -1.341 0.182 术后1月 63.1±4.0 65.0±4.3 2.506 0.014 t 2.661 -1.082 P 0.009 0.282 CD4+(%) 术前 38.8±3.0 38.1±2.6 -1.366 0.175 术后1月 38.2±3.1 39.4±2.9 2.190 0.031 t 1.077 -2.585 P 0.284 0.011 CD8+(%) 术前 23.0±2.1 23.3±1.8 0.840 0.403 术后1月 23.5±2.4 23.0±2.1 -1.214 0.227 t -1.214 0.840 P 0.227 0.403 CD4+/CD8+ 术前 1.69±0.18 1.64±0.16 -1.608 0.110 术后1月 1.63±0.20 1.71±0.17 2.361 0.020 t 1.727 -2.323 P 0.087 0.022
下载: 导出CSV
表 4 两组患儿生活质量评分比较
Table 4. Comparison of the quality of life scores between the two groups of children(n=60, Mean±SD)
因素 全切组 非全切组 t P 睡眠紊乱 术前 5.10±0.83 4.94±0.90 1.012 0.313 术后1月 2.36±0.61 2.50±0.73 -1.14 0.257 t 20.605 16.310 P 0.000 0.000 身体症状 术前 4.98±0.90 4.70±0.94 1.667 0.098 术后1月 3.13±0.77 3.37±0.81 -1.663 0.099 t 12.099 8.303 P 0.000 0.000 情绪影响 术前 4.47±0.80 4.24±0.92 1.461 0.147 术后1月 2.14±0.65 2.34±0.82 -1.481 0.141 t 17.509 11.942 P 0.000 0.000 白天问题 术前 4.18±0.63 4.00±0.78 1.391 0.167 术后1月 2.00±0.49 2.20±0.62 -1.96 0.052 t 21.157 13.993 P 0.000 0.000 看护者关心 术前 3.72±0.67 3.94±0.74 -1.707 0.09 术后1月 1.84±0.52 2.01±0.66 -1.567 0.12 t 17.17 15.077 P 0.000 0.000
下载: 导出CSV
表 5 两组患儿睡眠参数比较
Table 5. Comparison of sleep parameters between the two groups of children(n=60, Mean±SD)
组别 AHI t P 最低血氧饱和度 t P 术前 术后1月 术前 术后1月 全切组 14.2±2.6 3.2±1.5 28.386 0.000 74.8±4.5 91.7±2.3 -25.903 0.000 非全切组 13.8±3.1 3.7±1.8 21.825 0.000 73.6±3.9 91.2±2.5 -29.429 0.000 t 0.766 -1.653 1.561 1.140 P 0.445 0.101 0.121 0.257
下载: 导出CSV
-
[1] 张亚梅, 赵靖, 刘卫一, 等. 儿童阻塞性睡眠呼吸暂停低通气综合征的诊治[J]. 中华耳鼻咽喉科杂志, 2004, 39(11): 654-7. https://www.cnki.com.cn/Article/CJFDTOTAL-ZHEB200411004.htm [2] 蔡谦, 苏振忠, 文卫平, 等. 儿童阻塞性睡眠呼吸暂停低通气综合征扁桃体腺样体评价[J]. 中国耳鼻咽喉头颈外科, 2006, 13(7): 437-40. doi: 10.3969/j.issn.1672-7002.2006.07.004 [3] 孙楷, 聂洪玉, 徐东兰, 等. 鼾症患者中阻塞性睡眠呼吸暂停低通气综合征的筛查及危险因素分析[J]. 中国呼吸与危重监护杂志, 2019, 18 (1): 26-30. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGHW201901008.htm [4] 周津徽, 张欣, 王成禹, 等. 低温等离子消融术治疗儿童阻塞性睡眠呼吸暂停低通气综合征的效果及对免疫功能的影响[J]. 中国医学文摘: 耳鼻咽喉科学, 2020, 35(6): 438-41. https://www.cnki.com.cn/Article/CJFDTOTAL-GDYY201706027.htm [5] 曾宪平, 陈晓明, 张洪涛, 等. 扁桃体部分切除术对OSAHS患儿的临床效果观察[J]. 中国临床解剖学杂志, 2020, 38(6): 719-22. https://www.cnki.com.cn/Article/CJFDTOTAL-ZLJZ202006019.htm [6] 唐晓旭, 王晓梅. 低温等离子扁桃体切除术治疗儿童OSAHS研究进展[J]. 人民军医, 2020, 63(12): 1235-9. doi: 10.3969/j.issn.1000-9736.2020.12.027 [7] Wanyan PP, Wang JQ, Wang WG, et al. Obstructive sleep apnea hypopnea syndrome: Protocol for the development of a core outcome set[J]. Medicine, 2020, 99(34): e21591. doi: 10.1097/MD.0000000000021591 [8] Liu CD, Wang HY, Zhu CB, et al. Plasma expression of HIF-1α as novel biomarker for the diagnosis of obstructive sleep apnea-hypopnea syndrome[J]. J Clin Lab Anal, 2020, 34(12): 23545-6. doi: 10.1002/jcla.23545 [9] Lu M, Fang F, Wang ZJ, et al. Association between serum/plasma levels of adiponectin and obstructive sleep apnea hypopnea syndrome: a meta-analysis[J]. Lipids Heal Dis, 2019, 18(1): 30. doi: 10.1186/s12944-019-0973-z [10] 高茜, 姜琳琳, 王丽妍, 等. 单纯鼾症与阻塞性睡眠呼吸暂停低通气综合征患者睡眠期间的有效通气量、血氧浓度及睡眠和生活质量的比较[J]. 医学临床研究, 2019, 36(4): 643-4, 647. doi: 10.3969/j.issn.1671-7171.2019.04.007 [11] 罗静, 苏庚. 鼻内窥镜下低温等离子射频术治疗小儿鼾症临床效果分析[J]. 当代医学, 2019, 25(4): 83-5. https://www.cnki.com.cn/Article/CJFDTOTAL-DDYI201904033.htm [12] 杨佳讯, 王志琴, 吴劲燕. 护理临床路径在低温等离子射频消融术治疗儿童扁桃体和腺样体肥大中的应用[J]. 中华危重症医学杂志: 电子版, 2020, 13(4): 319-20. doi: 10.3877/cma.j.issn.1674-6880.2020.04.018 [13] 郭虹, 贾贵兰. 多平面低温等离子射频消融术治疗中重度阻塞性睡眠呼吸暂停低通气综合征的术后护理研究[J]. 世界睡眠医学杂志, 2019, 6(6): 832-3. doi: 10.3969/j.issn.2095-7130.2019.06.062 [14] 戴宁, 徐东亮. 不同手术方式对儿童OSHAS相关指标与通气功能的影响[J]. 中国中西医结合耳鼻咽喉科杂志, 2020, 28(1): 40-3, 69. https://www.cnki.com.cn/Article/CJFDTOTAL-XYJH202001009.htm [15] Liu Y, Han J, Ning L, et al. Cognitive function and life quality of patients with moderate-to-severe obstructive sleep apnea-hypopnea syndrome in China[J]. Expert Rev Respir Med, 2021, 15(3): 435-40. http://www.researchgate.net/publication/347630788_Cognitive_function_and_life_quality_of_patients_with_moderate-to-severe_obstructive_sleep_apnea-hypopnea_syndrome_in_China [16] Wang X, Liu Y, Tang G, et al. Effects of low-temperature plasma treatment on pulmonary function in children with obstructive sleep apnea-hypopnea syndrome[J]. Ir J Med Sci, 2020, 189(2): 603-9. doi: 10.1007/s11845-019-02132-2 [17] Song B, Li Y, Sun J, et al. Computational fluid dynamics simulation of changes in the morphology and airflow dynamics of the upper airways in OSAHS patients after treatment with oral appliances[J]. PLoS One, 2019, 14(11): e0219642. doi: 10.1371/journal.pone.0219642 [18] Hua F, Zhao TT, Walsh T, et al. Effects of adenotonsillectomy on the growth of children with obstructive sleep apnoea-hypopnea syndrome (OSAHS): protocol for a systematic review[J]. BMJ Open, 2019, 9(8): e030866. http://bmjopen.bmj.com/content/9/8/e030866.full [19] Zybleva SV, Zyblev SL, . The dynamics of CD3 + CD4 + CD8 + T-lymphocytes in kidney transplant recipients in the early and late post-transplantation period[J]. Vestnik VSMU, 2020, 19(1): 73-9. http://www.researchgate.net/publication/339481760_The_dynamics_of_CD3_CD4_CD8_T-lymphocytes_in_kidney_transplant_recipients_in_the_early_and_late_post-transplantation_period [20] Gao M, Liu Y, Guo M, et al. Regulatory CD4+ and CD8+ T cells are negatively correlated with CD4+ /CD8+ T cell ratios in patients acutely infected with SARS-CoV-2[J]. J Leukoc Biol, 2021, 109 (1): 91-7. http://www.researchgate.net/publication/344286395_Regulatory_CD4_and_CD8_T_cells_are_negatively_correlated_with_CD4_CD8_T_cell_ratios_in_patients_acutely_infected_with_SARS-CoV-2 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 215
- HTML全文浏览量: 96
- PDF下载量: 2
- 被引次数: 0