



Application of intraoperative awake anesthesia combined with multimodal images in reoperation of patients with recurrent glioma: 20 cases of two-year follow-up study
-
摘要:
目的观察术中唤醒麻醉联合多模态影像在切除脑复发胶质瘤患者手术中的作用和疗效。 方法回顾分析2017年1月~ 2020年12月广东药科大学附属第一医院神经外科20例再次手术切除的脑复发胶质瘤患者的临床资料,根据手术方式分为唤醒麻醉组(n=6)和常规手术组(n=14)。两组术中均根据术前功能磁共振神经影像导航引导下,通过皮层电刺激技术定位语言或运动皮层区域,在荧光显微镜下根据肿瘤荧光显影范围切除肿瘤。使用3D-slicer软件评估肿瘤切除程度;利用简易智力状况检查及Karnofsky功能状态评分比较患者术前、术后1周的认知功能和生活状态,随访1次/3月。 结果20例患者的复发时间14.65± 7.64月。所有手术均顺利进行,唤醒麻醉组患者完全配合术者指令动作,术中电刺激确定语言功能区1例,运动功能区1例。术后病理均为胶质母细胞瘤,WHO Ⅳ级。根据3D-slicer软件测量,唤醒麻醉组肿瘤减负率高于常规手术组(P < 0.05)。唤醒麻醉组无术后并发症及死亡病例,常规手术组出现神经功能近期障碍者1例。常规手术组患者术后1周的简易智力状况检查评分、Karnofsky功能状态评分较术前明显降低(P < 0.05),唤醒麻醉组各指标差异无统计学意义(P > 0.05)。两组患者随访时间为3~24月,两组间无进展生存率和总生存率差异无统计学意义(P > 0.05)。 结论术中唤醒麻醉结合多模态影像有助于在保护患者神经功能的前提下,最大化切除脑复发胶质瘤,为保障患者再次手术后的生活质量提供了一种安全的手术策略。 Abstract:ObjectiveTo observe the effect of intraoperative awake anesthesia combined with multimodal images in the resection of recurrent glioma. MethodsThe clinical data of 20 patients with recurrent glioma who underwent reoperation in our hospital from January 2017 to December 2020 were retrospectively analyzed. They were divided into awake anesthesia group (n=6) and conventional operation group (n=14). Under the guidance of preoperative fMRI neuronavigation, the language or motor cortex was located by cortical electrical stimulation technology, and the tumor was removed under fluorescence microscope. 3D-slicer software was used to evaluate the extent of tumor resection. Mini mental state examination and Karnofsky functional state score were used to compare the cognitive function and life status of patients before and 1 week after surgery. Follow-up was conducted every 3 months. ResultsTwenty patients with recurrent gliomas were selected for reoperation, the average recurrence time was 14.65±7.64 months. There was no significant difference in preoperative baseline data between the two groups (P > 0.05). All the operations were carried out smoothly. In the awake anesthesia group, the patients fully cooperated with the operator's instructions. During the operation, 1 case of language functional area and 1 case of motor functional area were confirmed by electrical stimulation. Postoperative pathology was glioblastoma, WHO grade IV. According to 3D-slicer software measurement, the tumor burden reduction rate of awake anesthesia group was significantly higher than that of conventional operation group (P < 0.05). There were no postoperative complications and death cases in the awake anesthesia group, but 1 case of recent neurological dysfunction occurred in the conventional operation group. The Mini mental state examination and Karnofsky functional state score in the conventional operation group were significantly lower than those before operation (P < 0.05), but there was no significant difference in the awake anesthesia group (P > 0.05). Follow-up time was 3~24 months, there was no significant difference in progression free survival and overall survival between the two groups (P > 0.05). ConclusionIntraoperative awake anesthesia combined with multimodal images is helpful to maximize the resection of brain recurrent gliomas on the premise of protecting patients' neurological function, and provides a safe surgical strategy for ensuring the quality of life of patients after reoperation. -
Key words:
- recurrent glioma /
- awake anesthesia /
- multimodal images /
- reoperation
-

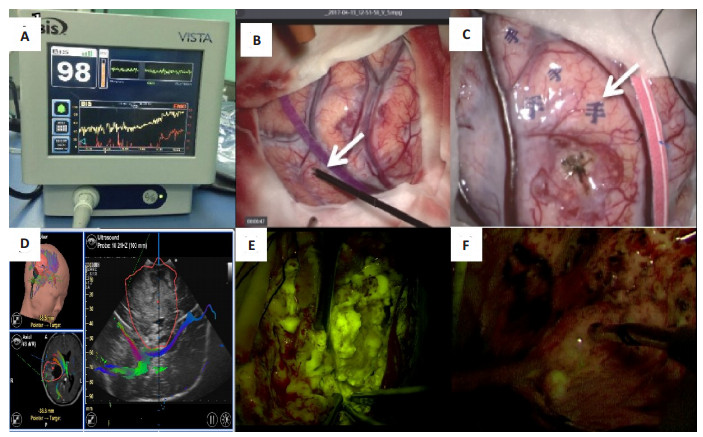
图 1 手术过程中患者意识监测及肿瘤定位情况
A:患者成功被唤醒后,BIS读数98;B:术中皮层电刺激定位脑功能区(白色箭头);C:神经电生理准确定位出手的运动中枢(白色箭头);D:神经导航结合术中B超可见神经纤维束位于肿瘤的内侧边缘;E:荧光显微镜下切除黄色荧光染色肿瘤;F:荧光显微镜下未见黄色荧光染色组织.
Figure 1. Consciousness monitoring and tumor location during operation.
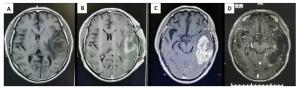
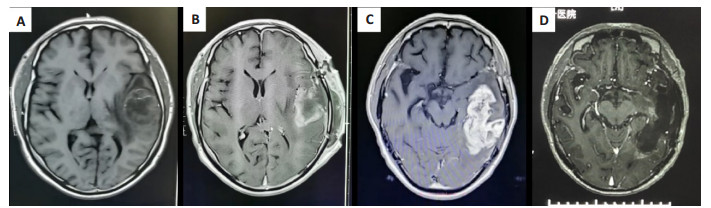
图 2 唤醒麻醉下复发胶质瘤的切除程度
A: 第1次手术前左侧颞叶占位,术后病理报间变性星形细胞瘤(WHO Ⅲ级);B: 术后72 h内复查头颅MR,肿瘤基本切除;C: 12月后复查考虑左侧颞叶肿瘤复发;D: 唤醒麻醉下再次手术切除肿瘤,术后病理报胶质母细胞瘤(WHO IV级).
Figure 2. Resection degree of recurrent glioma under awake anesthesia.

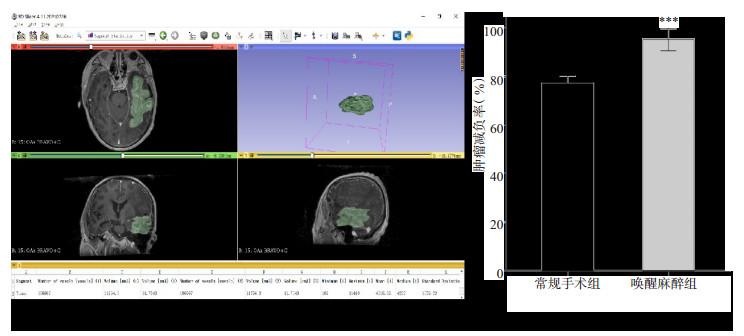
图 3 3D-slicer绘制肿瘤体积
Figure 3. The tumor volume was calculated by 3D-slicer. ***P < 0.01.

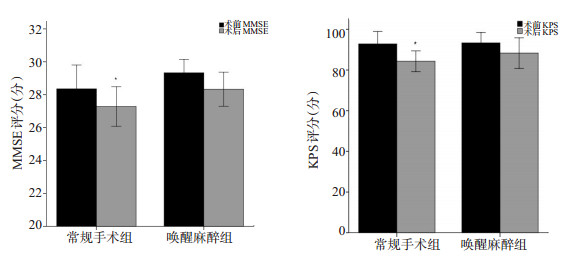
图 4 两组患者手术前及术后MMSE、KPS评分对比
Figure 4. Comparison in MMSE, KPS before and after operation between the two group. *P < 0.05.

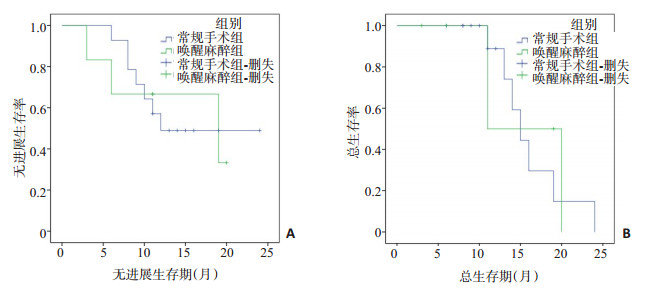
图 5 两组复发脑胶质瘤患者无进展生存率(A)和总生存率(B)的Kaplan Meier生存曲线图
Figure 5. Kaplan Meier survival curve of progression free survival (A) and overall survival (B) in two groups of patients with recurrent glioma.
表 1 两组患者一般资料对比
Table 1. The baseline data in two groups of patients (Mean±SD)
分组 年龄(岁) 男/女(n) 复发时间(月) 术前MMSE评分(分) 术前KPS评分(分) 常规手术组(n=14) 49.07±11.11 9月5日 16±7.97 28.35±1.45 92.86±6.11 唤醒麻醉组(n=6) 46.50±9.44 5月1日 11.5±6.28 29.33±0.82 93.33±5.16  下载: 导出CSV
下载: 导出CSV
-
[1] Porter KR, McCarthy BJ, Freels S, et al. Prevalence estimates for primary brain tumors in the United States by age, gender, behavior, and histology[J]. Neuro Oncol, 2010, 12(6): 520-7. doi: 10.1093/neuonc/nop066 [2] Vincenzo Barbagallo GM, Certo F, Di Gregorio S, et al. Recurrent high-grade glioma surgery: a multimodal intraoperative protocol to safely increase extent of tumor resection and analysis of its impact on patient outcome[J]. Neurosurg Focus, 2021, 50(1): E20. doi: 10.3171/2020.10.FOCUS20744 [3] 白红民, 王伟民, 梁树杰, 等. 脑功能区胶质瘤的现代手术策略[J]. 临床神经外科杂志, 2011, 8(5): 245-8. doi: 10.3969/j.issn.1672-7770.2011.05.007 [4] 严勇, 王洪祥, 徐涛, 等. 多中心脑胶质瘤诊治的临床研究[J]. 中华医学杂志, 2015, 95(13): 991-5. doi: 10.3760/cma.j.issn.0376-2491.2015.13.008 [5] Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma[J]. N Engl J Med, 2005, 352(10): 987-96. doi: 10.1056/NEJMoa043330 [6] Stupp R, Hegi ME, Mason WP, et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase Ⅲ study: 5-year analysis of the EORTC-NCIC trial[J]. Lancet Oncol, 2009, 10(5): 459-66. doi: 10.1016/S1470-2045(09)70025-7 [7] Hickmann AK, Nadji-Ohl M, Hopf NJ. Feasibility of fluorescence-guided resection of recurrent gliomas using five-aminolevulinic acid: retrospective analysis of surgical and neurological outcome in 58 patients[J]. J Neurooncol, 2015, 122(1): 151-60. doi: 10.1007/s11060-014-1694-9 [8] 库格鲁克·亚力坤, 周庆九. 复发性胶质瘤的治疗进展[J]. 临床神经外科杂志, 2020, 17(5): 588-91. doi: 10.3969/j.issn.1672-7770.2020.05.023 [9] McGirt MJ, Mukherjee D, Chaichana KL, et al. Association of surgically acquired motor and language deficits on overall survival after resection of glioblastoma multiforme[J]. Neurosurgery, 2009, 65(3): 463-70. doi: 10.1227/01.NEU.0000349763.42238.E9 [10] Chaichana KL, Chaichana KK, Olivi A, et al. Surgical outcomes for older patients with glioblastoma multiforme: preoperative factors associated with decreased survival. Clinical article[J]. J Neurosurg, 2011, 114(3): 587-94. doi: 10.3171/2010.8.JNS1081 [11] McGirt MJ, Chaichana KL, Gathinji M, et al. Independent association of extent of resection with survival in patients with malignant brain astrocytoma[J]. J Neurosurg, 2009, 110(1): 156-62. doi: 10.3171/2008.4.17536 [12] Chaichana KL, Zadnik P, Weingart JD, et al. Multiple resections for patients with glioblastoma: prolonging survival[J]. J Neurosurg, 2013, 118(4): 812-20. doi: 10.3171/2012.9.JNS1277 [13] Sanai N, Mirzadeh Z, Berger MS. Functional outcome after language mapping for glioma resection[J]. N Engl J Med, 2008, 358 (1): 18-27. doi: 10.1056/NEJMoa067819 [14] So EL, Alwaki A. A guide for cortical electrical stimulation mapping [J]. J Clin Neurophysiol, 2018, 35(2): 98-105. doi: 10.1097/WNP.0000000000000435 [15] 吴斌, 路俊锋, 章捷, 等. 多模态技术联合术中唤醒麻醉在broca区胶质瘤患者语言功能区定位中的作用[J]. 中华神经外科杂志, 2020, 36 (2): 124-9. [16] 鲁明, 周辉, 邓星海, 等. 术中唤醒麻醉下切除颅内病变的临床观察(附200例报告)[J]. 中华神经外科杂志, 2017, 33(3): 275-9. doi: 10.3760/cma.j.issn.1001-2346.2017.03.011 [17] 苏海波, 张玲琼, 陈保东, 等. 术中唤醒结合神经导航在脑功能区胶质瘤手术中的应用价值分析[J]. 中华神经医学杂志, 2020, 19(6): 546-51. doi: 10.3760/cma.j.cn115354-20191018-00601 [18] Broekx S, Weyns F, De Vleeschouwer S. 5-Aminolevulinic acid for recurrent malignant gliomas: a systematic review[J]. Clin Neurol Neurosurg, 2020, 195: 105913. doi: 10.1016/j.clineuro.2020.105913 [19] Stummer W, Pichlmeier U, Meinel T, et al. Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: a randomised controlled multicentre phase Ⅲ trial[J]. Lancet Oncol, 2006, 7(5): 392-401. doi: 10.1016/S1470-2045(06)70665-9 [20] 黄进, 张晓路, 张岩松, 等. 多模态神经导航联合术中荧光导向技术在脑功能区高级别胶质瘤中的应用[J]. 南京医科大学学报: 自然科学版, 2018, 38(1): 14-9. https://www.cnki.com.cn/Article/CJFDTOTAL-NJYK201801005.htm [21] Lu VM, Phan K, Rovin RA. Comparison of operative outcomes of eloquent glioma resection performed under awake versus general anesthesia: a systematic review and meta-analysis[J]. Clin Neurol Neurosurg, 2018, 169: 121-7. doi: 10.1016/j.clineuro.2018.04.011 [22] Gravesteijn BY, Keizer ME, Vincent AJPE, et al. Awake craniotomy versus craniotomy under general anesthesia for the surgical treatment of insular glioma: choices and outcomes[J]. Neurol Res, 2018, 40(2): 87-96. doi: 10.1080/01616412.2017.1402147 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 407
- HTML全文浏览量: 133
- PDF下载量: 9
- 被引次数: 0