



Correlation between UtA-PI, UtA-RI and S/D values measured by ultrasound in different pregnancy periods and the prediction of the condition of pregnant women with hypertension in pregnancy and the maternal and infant outcome Screening Fetal Down's Syndrome
-
摘要:
目的分析不同孕期孕产妇患者超声测定的子宫动脉搏动指数(UtA-PI)、阻力指数(UtA-RI)和S/D值与妊娠期高血压疾病(HDCP)孕妇病情预测及母婴结局的相关性。 方法选择我院2018年1月~2019年12月间收治的162例符合纳入标准的HDCP患者作为观察组,正常妊娠孕妇100例作为对照组。妊娠早期(10~14周)、妊娠中期(20~23周)、妊娠晚期(30~31周)行超声检查并记录UtA-PI、UtA-RI和S/D;用logistics回归模型分析UtA-PI、UtA-RI和S/D值与HDCP孕妇母婴结局关系,绘制ROC曲线分析UtA-PI、UtA-RI和S/D值预测HDCP的价值。 结果妊娠中期和妊娠晚期,观察组UtA-PI、UtA-RI和S/D值均高于对照组(P < 0.05);妊娠中期和妊娠晚期,超声检查UtA-PI、UtA-RI和S/D值鉴别诊断HDCP的敏感度和特异度均高于85%,且AUC均大于0.9;妊娠中期和妊娠按期妊娠异常组HDCP孕妇UtA-PI、UtA-RI和S/D值均高于正常妊娠组(P < 0.05);妊娠中期和妊娠晚期,HDCP孕妇超声检查的UtA-PI、UtA-RI和S/D值均是影响妊娠结局的独立性威胁因素(P < 0.05)。 结论超声测定孕妇UtA-PI、UtA-RI和S/D值可有效预测HDCP,且UtA-PI、UtA-RI和S/D值是影响妊娠结局的独立性威胁因素。 Abstract:ObjectiveTo analyze the correlation between the UtA-PI, UtA-RI and S/D values measured by ultrasound in pregnant women of different pregnancy periods and the hypertensive disorder complicating pregnant (HDCP) women's disease prediction and maternal and infant outcomes. MethodsA total of 162 HDCP patients who reach the inclusion criteria from January 2018 to December 2019 in our hospital were selected as the observation group, and 100 normal pregnant women were used as the control group. Ultrasound examination was performed in the first trimester (10-14 weeks), the second trimester (20-23 weeks), and the third trimester (30-31 weeks) to record UtA-PI, UtA-RI and S/D. The relationship between UTA PI, UTA RI and S/D was analyzed by logistic regression model. The ROC curve was used to analyze the value of UTA PI, UTA RI and S/D in predicting HDCP. ResultsThe UtA-PI, UtA-RI and S/D values of the observation group during the second and third trimester were significantly higher than those of the control group, and the difference was significant (P<0.05). The sensitivity and specificity of UtA-RI and S/D values for differential diagnosis of HDCP are higher than 85%, and the AUC was greater than 0.9. The values of UtA-PI, UtA-RI and S/D of HDCP pregnant women in the second and third trimester pregnancy abnormal pregnancy groups were higher than those of normal pregnancy group (P<0.05). UtA-PI, UtA-RI and S/D values of ultrasonography of HDCP pregnant women during the second and third trimesters were independent of the outcome of pregnancy Threats (P<0.05). ConclusionThe value of UTA-PI, UTA-RI and S/D measured by ultrasound can effectively predict HDCP. The value of UTA-PI, UTA-RI and S/D are independent threat factors affecting pregnancy outcome. -

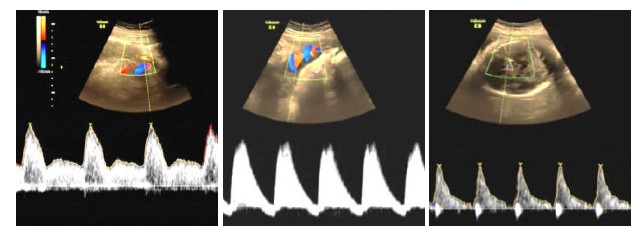
图 1 子宫动脉血流、脐动脉血流、胎儿大脑中动脉血流频谱病理图片
Figure 1. Pathological pictures of uterine artery blood flow, umbilical artery blood flow, and fetal middle cerebral artery blood flow spectrum.
表 1 两组UtA-PI、UtA-RI和S/D值检测结果
Table 1. Detection results of two groups of UtA-PI, UtA-RI and S/D value (Mean±SD)
组别 UtA-PI UtA-RI S/D 早期 观察组(n=162) 1.48±0.61 0.71±0.26 3.33±0.31 对照组(n=100) 1.33±0.58 0.69±0.34 3.21±0.29 t 1.182 0.537 0.520 P 0.238 0.592 0.604 中期 观察组(n=162) 1.49±0.35 0.78±0.21 3.59±0.28 对照组(n=100) 1.15±0.24 0.55±0.19 2.56±0.24 t 8.550 8.296 30.508 P < 0.001 < 0.001 < 0.001 晚期 观察组(n=162) 1.21±0.19 0.59±0.15 3.15±0.21 对照组(n=100) 0.95±0.13 0.42±0.16 2.12±0.13 t 12.049 8.687 44.091 P < 0.001 < 0.001 < 0.001 UtA-PI: 子宫动脉搏动指数; UtA-RI: 子宫动脉阻力指数.  下载: 导出CSV
下载: 导出CSV
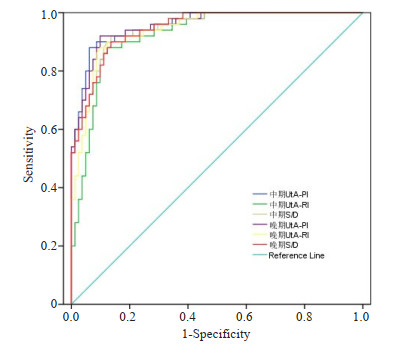
表 2 中期和晚期妊娠鉴别诊断HDCP孕妇结果
Table 2. Results of the differential diagnosis of HDCP pregnant women in the second and third trimester (%)
指标 敏感度 特异性 AUC 中期 UtA-PI 92.59(150/162) 88.00(88/100) 0.957 UtA-RI 89.51(145/162) 87.00(87/100) 0.922 S/D 88.27(143/162) 89.00(89/100) 0.946 晚期 UtA-PI 90.74(147/162) 90.00(90/100) 0.955 UtA-RI 89.51(145/162) 88.00(88/100) 0.941 S/D 87.65(142/162) 89.00(89/100) 0.946 HDCP: 妊娠期高血压疾病.
下载: 导出CSV
表 3 不同妊娠结局HDCP孕妇各指标检测结果
Table 3. Test results of various indicators of HDCP pregnant women with different pregnancy outcomes (Mean±SD)
组别 UtA-PI UtA-RI S/D 早期 正常(n=103) 1.47±0.59 0.70±0.51 3.31±0.28 异常(n=59) 1.50±0.62 0.73±0.45 3.36±0.31 t 0.306 0.376 1.052 P 0.760 0.708 0.295 中期 正常(n=103) 1.39±0.37 0.71±0.13 3.11±0.21 异常(n=59) 1.66±0.29 0.90±0.11 4.43±0.19 t 4.819 9.451 39.830 P < 0.001 < 0.001 < 0.001 晚期 正常(n=103) 1.12±0.26 0.54±0.16 2.96±0.15 异常(n=59) 1.37±0.31 0.68±0.12 3.48±0.13 t 5.485 5.842 22.260 P < 0.001 < 0.001 < 0.001
下载: 导出CSV
表 4 HDCP孕妇各指标与妊娠结局关系
Table 4. The relationship between the indicators of HDCP pregnant women and pregnancy outcome
指标 b SE χ2 P OR 95%CI 上限 下限 中期 UtA-PI 0.634 0.237 7.156 0.007 1.885 1.185 3.000 UtA-RI 0.575 0.215 7.153 0.007 1.777 1.166 2.709 S/D 0.613 0.208 8.685 0.003 1.846 1.228 2.775 晚期 UtA-PI 0.551 0.225 5.997 0.014 1.735 1.116 2.697 UtA-RI 0.635 0.216 8.643 0.003 1.887 1.236 2.882 S/D 0.612 0.259 5.583 0.018 1.844 1.110 3.064
下载: 导出CSV
-
[1] Johnson P, Montgomery M, Ewell P. Elevated blood pressure in lowincome, rural preschool children is associated with maternal hypertension during pregnancy[J]. J Community Health Nurs, 2018, 35(1): 12-8. doi: 10.1080/07370016.2018.1404830 [2] Lundgren SN, Madan JC, Emond JA, et al. Maternal diet during pregnancy is related with the infant stool microbiome in a delivery mode-dependent manner[J]. Microbiome, 2018, 6(1): 109. doi: 10.1186/s40168-018-0490-8 [3] Long JL, Xia W, Li JF, et al. Maternal urinary benzophenones and infant birth size: Identifying critical windows of exposure[J]. Chemosphere, 2019, 219: 655-61. doi: 10.1016/j.chemosphere.2018.11.190 [4] 庞静, 聂红艳, 陈伟伟, 等. 妊娠期高血压疾病产妇子宫动脉和胎儿脐动脉超声参数预测妊娠结局的临床价值[J]. 中国计划生育和妇产科, 2019, 11(1): 77-80, 97. https://www.cnki.com.cn/Article/CJFDTOTAL-JHFC201901021.htm [5] Roth DE, Morris SK, Zlotkin S, et al. Vitamin D supplementation in pregnancy and lactation and infant growth[J]. N Engl J Med, 2018, 379(6): 535-46. doi: 10.1056/NEJMoa1800927 [6] Torlinska B, Bath SC, Janjua A, et al. Iodine status during pregnancy in a region of mild-to-moderate iodine deficiency is not associated with adverse obstetric outcomes; results from the Avon longitudinal study of parents and children (ALSPAC)[J]. Nutrients, 2018, 10(3): E291. doi: 10.3390/nu10030291 [7] 中华医学会妇产科学分会妊娠期高血压疾病学组. 妊娠期高血压疾病诊治指南(2015)[J]. 中华围产医学杂志, 2016, 19(3): 161-9. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGSF201510002.htm [8] Wheeler BJ, Taylor BJ, de Lange M, et al. A longitudinal study of 25- hydroxy vitamin D and parathyroid hormone status throughout pregnancy and exclusive lactation in new Zealand mothers and their infants at 45° S[J]. Nutrients, 2018, 10(1): E86. doi: 10.3390/nu10010086 [9] Ocansey ME, Pulakka A, Adu- Afarwuah S, et al. The effects of supplementing maternal and infant diets with lipid-based nutrient supplements on physical activity and sedentary behaviour at preschool age in Ghana[J]. Br J Nutr, 2019, 122(8): 884-94. doi: 10.1017/S0007114519001636 [10] 祝建芳, 韩星, 刘小如. 动态血压监测联合硝酸甘油对HDCP的治疗效果分析[J]. 西南国防医药, 2019, 29(3): 378-80. https://www.cnki.com.cn/Article/CJFDTOTAL-XNGF201903030.htm [11] Noor N, Ferguson KK, Meeker JD, et al. Pregnancy phthalate metabolite concentrations and infant birth weight by gradations of maternal glucose tolerance[J]. Int J Hyg Environ Health, 2019, 222 (3): 395-401. doi: 10.1016/j.ijheh.2018.12.005 [12] Donowitz JR, Cook H, Alam M, et al. Role of maternal health and infant inflammation in nutritional and neurodevelopmental outcomes of two-year-old Bangladeshi children[J]. PLoS Negl Trop Dis, 2018, 12(5): e0006363. doi: 10.1371/journal.pntd.0006363 [13] 巴哈尔古丽·阿不来提, 玛依拉·买买提, 祖丽皮亚·依明, 等. 妊娠期高血压疾病的相关危险因素及其严重程度对母婴结局的影响[J]. 中国妇幼保健, 2018, 33(19): 4380-3. https://www.cnki.com.cn/Article/CJFDTOTAL-ZFYB201819020.htm [14] Toly VB, Blanchette JE, Liu W, et al. Maternal stress and mental health prior to their technology-dependent infant's discharge home from the NICU[J]. J Perinat Neonatal Nurs, 2019, 33(2): 149-59. doi: 10.1097/JPN.0000000000000409 [15] Li W, Xu B, Cao Y, et al. Association of maternal folate intake during pregnancy with infant asthma risk[J]. Sci Rep, 2019, 9(1): 8347. doi: 10.1038/s41598-019-44794-z [16] Hardt U, Larsson A, Gunnarsson I, et al. Autoimmune reactivity to malondialdehyde adducts in systemic lupus erythematosus is associated with disease activity and nephritis[J]. Arthritis Res Ther, 2018, 20(1): 36. doi: 10.1186/s13075-018-1530-2 [17] Choi J, Summers W, Paszkowski U. Mechanisms underlying establishment of arbuscular mycorrhizal symbioses[J]. Annu Rev Phytopathol, 2018, 56: 135-60. doi: 10.1146/annurev-phyto-080516-035521 [18] 王扬. 硝苯地平对妊娠高血压患者脐动脉血流、围产结局及血小板指标的影响[J]. 血栓与止血学, 2018, 24(5): 812-4. https://www.cnki.com.cn/Article/CJFDTOTAL-XSZX201805030.htm [19] 杨丽君, 陈朝霞, 肖会能. 持续质量改进对妊娠期高血压孕产妇血压控制及母婴结局的护理干预研究[J]. 成都医学院学报, 2019, 14(4): 490-3. https://www.cnki.com.cn/Article/CJFDTOTAL-CDYU201904020.htm [20] Killock D. ARAMIS-is darolutamide set to become the 'third musketeer' of nmCRPC[J]? Nat Rev Clin Oncol, 2019, 16(5): 273. http://www.ncbi.nlm.nih.gov/pubmed/30809027 [21] Saito T, Saito Y, Fukumoto KJ, et al. Clinical and pathological characteristics of spontaneous pneumothorax in women: a 25-year single-institutional experience[J]. Gen Thorac Cardiovasc Surg, 2018, 66(9): 516-22. http://europepmc.org/abstract/MED/29846876 [22] 邵倩. 彩色多普勒超声诊断妊娠期高血压孕妇胎儿血流变化的临床意义[J]. 中国计划生育学杂志, 2019, 27(3): 394-5, 399. https://www.cnki.com.cn/Article/CJFDTOTAL-JHSY201903033.htm -

 点击查看大图
点击查看大图
计量
- 文章访问数: 512
- HTML全文浏览量: 422
- PDF下载量: 9
- 被引次数: 0