



Correlation between language impairment and cholinergic pathway damage in patients with acute basal ganglia infarction
-
摘要:
目的探讨不同程度的胆碱能通路损害对基底节区脑梗塞患者语言功能的影响。 方法纳入2018年10月~2020年10月神经内科住院的初次发病并伴有语言障碍的急性基底节区脑梗塞患者135例,所有患者均进行胆碱能通路高信号评分量表(CHIPS)检查,根据评分高低分为A组(轻度异常,CHIPS评分1~3分,n=42)、B组(中度异常,CHIPS评分4~7分,n=53)和C组(重度异常,CHIPS评分≥8,n=40),对3组患者分别实施标准汉语失语量表(ABC)检查,并运用Logistic回归寻找伴胆碱能通路损害的基底节区脑梗塞患者语言损害的相关因素;对3组患者的标准汉语失语量表各计算项目行单向方差分析,评估3组患者ABC量表各分项目得分的差异性。 结果ABC量表包括谈话、理解、复述、命名、阅读、书写、结构与视空间、运用、计算等项目,A组得分为25.05±1.72、204.67±5.14、91.36±5.19、78.31±2.34、50.48±4.56、87.07±3.22、14.48±1.31、27.31±1.89、22.24±1.67);B组得分为18.51±1.35、198.85±8.68、86.94±3.77、76.57±2.43、46.64±3.65、85.21±3.25、13.62±1.24、28.08±1.82、22.19±1.42;C组得分为16.35±2.09、195.42±7.03、85.95±2.88、72.93±4.23、44.35±3.41、83.58±2.91、12.73±2.17、27.80±1.78、21.85±1.71。经单因素方差分析,在谈话、理解、命名、阅读、书写、结构与视空间6个项目得分差异有统计学意义(P < 0.05);C组与A组的复述项目差异有统计学意义(P < 0.05),C组与B组差异无统计学意义(P=0.244);3组在运用、计算项目得分差异无统计学意义(P>0.05)。回归分析发现年龄、高同型半胱氨酸及梗塞体积是梗塞患者出现语言功能损害的危险因素(P < 0.05)。 结论基底节区脑梗塞患者语言损害的程度可能与其胆碱能通路的损害程度相关,年龄、高同型半胱氨酸及梗塞体积为基底节区脑梗塞患者出现语言功能损害的危险因素。 -
关键词:
- 基底节区脑梗塞 /
- 失语 /
- 胆碱能通路 /
- 标准汉语失语检查量表
Abstract:ObjectiveTo investigate the influence of different degrees of cholinergic pathway damage on the language function of patients with cerebral infarction in the basal ganglia. MethodsWe included 135 cases of acute basal ganglia cerebral infarction with initial onset and speech disorder in the Department of Neurology from October 2018 to October 2020. All patients were operated with the Cholinergic Pathway High Signal Scale (CHIPS) Check, according to the score. They were divided into group A (mild abnormality, CHIPS score 1-3 points, 42 cases), group B (moderate abnormality, CHIPS score 4-7 points, 53 cases) and group C (severe abnormality, CHIPS score ≥8, 40 cases). Three groups of patients were tested with the standard Chinese Aphasia Scale (ABC). Logistic regression was used to find the related factors of language damage in patients with basal ganglia cerebral infarction with cholinergic pathway damage. One-way analysis of variance was performed on each calculation item of the standard Chinese Aphasia Scale of the three groups of patients to evaluate the differences in the scores of the ABC scales of the three groups. ResultsABC scale score: (talk; comprehension; retelling; naming; reading; writing; structure and visual space; application; calculation): Group A (25.05±1.72; 204.67±5.14; 91.36±5.19; 78.31±2.34; 50.48±4.56; 87.07± 3.22; 14.48±1.31; 27.31±1.89; 22.24±1.67); Group B (18.51±1.35; 198.85±8.68; 86.94±3.77; 76.57±2.43; 46.3.25±3.65; 85.21±3.65; 1.24; 28.08±1.82; 22.19±1.42); Group C (16.35±2.09; 195.42±7.03; 85.95±2.88; 72.93±4.23; 44.35±3.41; 83.58±2.91; 12.73±2.17; 27.80±1.78; 21.85 ± 1.71). After one-way analysis of variance comparison, there are differences in the scores of 6 items in conversation, comprehension, naming, reading, writing, structure and visual space Statistical significance among three groups. In the retelling item, the difference between group C and group A was significant, and the difference between group C and group B was not significant (P=0.244). There was no significant difference in the scores of the three groups in use and calculation. Regression analysis found that age, high homocysteine, and infarct volume were risk factors for language impairment. ConclusionThe degree of language impairment in patients with cerebral infarction in the basal ganglia may be related to the degree of damage in the cholinergic pathway. Age, high homocysteine and infarct volume are risk factors for language impairment in patients with cerebral infarction in the basal ganglia. -
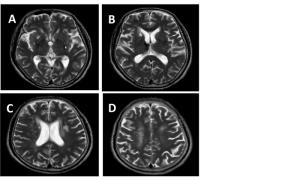
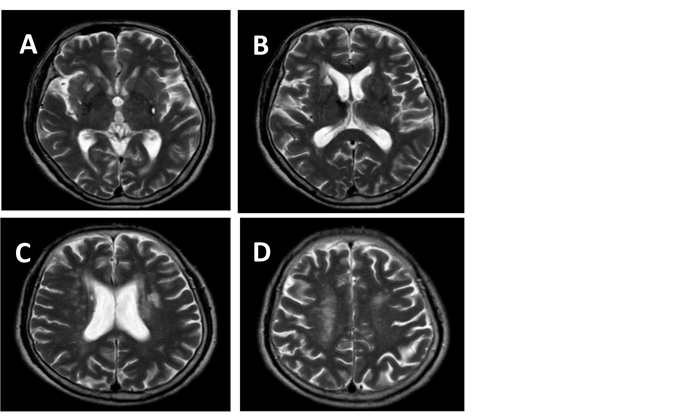
图 1 胆碱能通路示意图
A: 低外囊层面; B: 高外囊层面; C: 放射冠层面; D: 半卵圆中心层面.
Figure 1. Schematic diagram of cholinergic pathway.

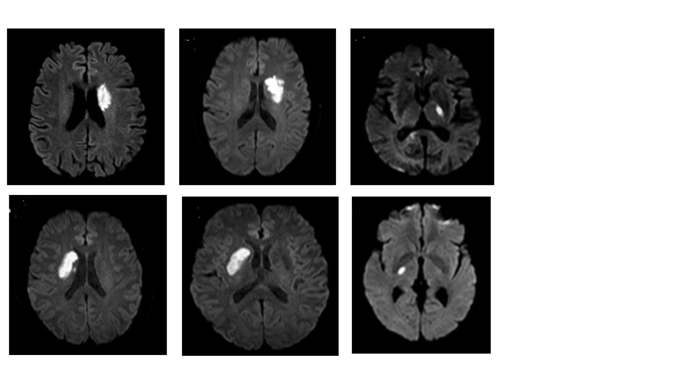
图 2 语言功能损害患者常见的梗塞位置
A: 左侧侧脑室; B: 右侧侧脑室; C: 左侧放射冠区; D: 右侧放射冠区; E: 左侧内囊后肢; F: 右侧内囊后肢.
Figure 2. High incidence of infarction in patients with language impairment.
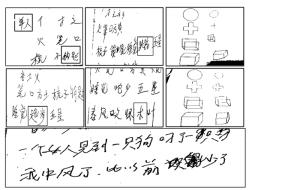
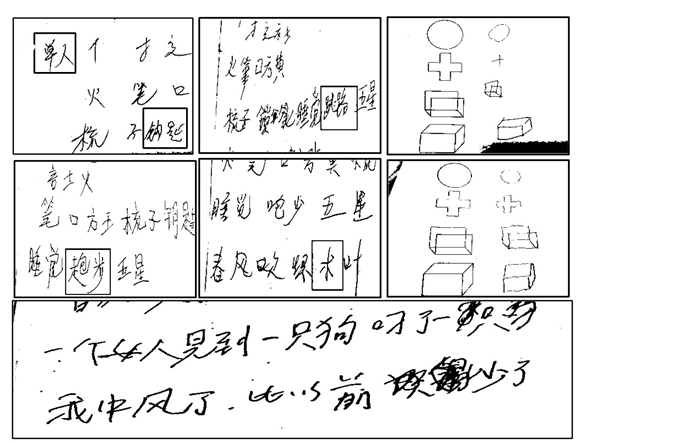
图 3 语言功能损害患者听写、空间画图及自主书写项目
A: 听写部首“亻”音译错写为“单人”“, 钥匙”字形错写; B、D: 听写“跑步”字形错写;E:听写“树”错写为“木”; C、F: 空间结构画图形状错误, 无法描绘出图形空间立体结构; G: 写病情项目中患者的语句结构简单, 缺乏主谓宾结构.
Figure 3. Dictation, spatial drawing and autonomous writing of patients with language impairment.
表 1 有语言功能损害与无语言功能损害组的临床特征比较
Table 1. Comparison of clinical features between Group with and without language impairment
指标 所有患者(n=202) 语言损害组(n=135) 非语言损害组(n=67) t/χ2 P 年龄(岁, Mean±SD) 64.13±9.59 66.97±8.30 58.40±9.52 8.95 0.003 收缩压(mmHg, Mean±SD) 154.24±14.06 154.71±14.58 153.13±12.61 0.37 0.546 舒张压(mmHg, Mean±SD) 86.12±4.72 86.36±4.86 85.63±4.44 0.43 0.514 高血糖(mmol/L, Mean±SD) 5.90±0.58 5.86± 0.56 5.97± 0.62 2.28 0.137 高LDL-C(mmol/L, Mean±SD) 3.30±2.15 3.42±0.40 3.06±0.69 4.37 0.038 高尿酸(μmol/L, Mean±SD) 286.28±80.07 290.10±82.08 278.56±75.87 2.41 0.122 高Hcy(mmol/L, Mean±SD) 13.87±4.14 14.96±3.65 11.68±4.23 5.05 0.026 梗塞体积(mm2, Mean±SD) 335.56±510.70 440.47±595.69 124.18±77.74 21.29 0.000 教育年限(年, Mean±SD) 7.45±2.58 7.32±1.68 8.65±2.21 1.85 0.216 性别[男, n(%)] 122(60.3) 81(60.0) 41 (61.1) 0.03 0.870 饮酒史[男, n(%)] 108(53.4) 79(58.5) 29(43.2) 4.17 0.041 吸烟史[男, n(%)] 112(55.4) 76(56.2) 36(53.73) 0.12 0.730 LDL-C: 低密度脂蛋白; Hcy: 同型半胱氨酸.  下载: 导出CSV
下载: 导出CSV
表 2 语言功能损害患者的相关影响因素Logistic回归分析
Table 2. Logistic regression analysis of related influencing factors in patients with language impairment
指标 P OR 95% 置信区间 下限 上限 年龄 0.000 0.871 0.820 0.924 饮酒史 0.124 1.928 0.835 4.452 梗塞体积 0.000 0.990 0.985 0.994 高血脂 0.660 1.031 0.901 1.180 高同型半胱氨酸 0.000 0.781 0.689 0.885 高尿酸 0.525 1.002 0.996 1.007
下载: 导出CSV
表 3 患者ABC量表评分比较
Table 3. Comparison of standard ChineseAphasia Checklist scores among the patients (Mean±SD)
指标 所有患者(n=135) A组(n=42) B组(n=53) C组(n=40) 谈话 19.90±3.96 25.05±1.72 18.51±1.35 16.35±2.09 理解 199.64±8.07 204.67±5.14 198.85±8.68 195.42±7.03 复述 88.02±4.63 91.36±5.19 86.94±3.77 85.95±2.88 命名 76.03±3.72 78.31±2.38 76.57±2.43 72.93±4.23 阅读 47.16±4.56 50.48±4.56 46.64±3.65 44.35±3.41 书写 85.30±3.40 87.07±3.22 85.21±3.25 83.58±2.91 结构与视空间 13.62±1.72 14.48±1.31 13.62±1.24 12.73±2.17 运用 27.76±1.85 27.31±1.89 28.08±1.82 27.80±1.78 计算 22.10±1.59 22.24±1.67 22.19±1.42 21.85±1.71 A组: 胆碱能通路轻度异常组; B组: 胆碱能通路中度异常组; C组: 胆碱能通路重度异常组.
下载: 导出CSV
表 4 患者的ABC评分量表各分项目得分方差分析
Table 4. Analysis of variance of each sub-item score of theABC scoring scale for the patients
评分项目 分组 P 95%置信区间 下限 上限 谈话 A组 B组 0.000 5.84 7.24 C组 A组 0.000 -9.45 -7.95 C组 B组 0.000 -2.87 -1.45 理解 A组 B组 0.000 2.86 8.78 C组 A组 0.000 -12.41 -6.07 C组 B组 0.026 -6.43 -0.42 复述 A组 B组 0.000 2.76 6.07 C组 A组 0.000 -7.18 -3.63 C组 B组 0.244 -2.67 0.69 阅读 A组 B组 0.000 2.24 5.43 C组 A组 0.000 -7.83 -4.42 C组 B组 0.006 -3.91 -0.68 命名 A组 B组 0.007 0.49 3.00 C组 A组 0.000 -6.72 -4.05 C组 B组 0.000 -4.91 -2.37 书写 A组 B组 0.005 0.58 3.15 C组 A组 0.000 -4.87 -2.13 C组 B组 0.014 -2.93 -0.33 结构与视空间 A组 B组 0.011 0.20 1.50 C组 A组 0.000 -2.45 -1.06 C组 B组 0.008 -1.56 -0.24 运用 A组 B组 0. 081 -1.43 0.08 C组 A组 0.229 -0.31 1.29 C组 B组 0.475 -1.04 0.49 计算 A组 B组 0.881 -0.60 0.70 C组 A组 0.285 -1.19 0.51 C组 B组 0.353 -1.21 0.74
下载: 导出CSV
-
[1] Cohen DL, Roffe C, Beavan J, et al. Post-stroke dysphagia: a review and design considerations for future trials[J]. Int J Stroke, 2016, 11(4): 399-411. doi: 10.1177/1747493016639057 [2] Sinanović O, Mrkonjić Z, Zukić S, et al. Post-stroke language disorders [J]. Acta Clin Croat, 2011, 50(1): 79-94. http://www.ncbi.nlm.nih.gov/pubmed/22034787 [3] Ali M, Lyden P, Brady M, et al. Aphasia and dysarthria in acute stroke: recovery and functional outcome[J]. Int J Stroke, 2015, 10(3): 400-6. doi: 10.1111/ijs.12067 [4] Ojemann G, Ojemann J, Lettich E, et al. Cortical language localization in left, dominant hemisphere. An electrical stimulation mapping investigation in 117 patients[J]. J Neurosurg, 1989, 71(3): 316-26. doi: 10.3171/jns.1989.71.3.0316 [5] Ojemann GA. Cortical organization of language[J]. J Neurosci, 1991, 11(8): 2281-7. doi: 10.1523/JNEUROSCI.11-08-02281.1991 [6] Whitwell JL, Duffy JR, Strand EA, et al. Distinct regional anatomic and functional correlates of neurodegenerative apraxia of speech and aphasia: an MRI and FDG-PET study[J]. Brain Lang, 2013, 125(3): 245-52. doi: 10.1016/j.bandl.2013.02.005 [7] Ivanova MV, Isaev DY, Dragoy OV, et al. Diffusion-tensor imaging of major white matter tracts and their role in language processing in aphasia[J]. Cortex, 2016, 85: 165-81. doi: 10.1016/j.cortex.2016.04.019 [8] Jiménez de la Peña MM, Gómez Vicente L, García Cobos R, et al. Neuroradiologic correlation with aphasias. Cortico-subcortical map of language[J]. Radiologia, 2018, 60(3): 250-61. doi: 10.1016/j.rx.2017.12.008 [9] Brady MC, Kelly H, Godwin J, et al. Speech and language therapy for aphasia following stroke[J]. Cochrane Database Syst Rev, 2016(6): CD000425. http://www.ncbi.nlm.nih.gov/pubmed/10796360 [10] Berthier ML, Green C, Higueras C, et al. A randomized, placebocontrolled study of donepezil in poststroke aphasia[J]. Neurology, 2006, 67(9): 1687-9. doi: 10.1212/01.wnl.0000242626.69666.e2 [11] Zhang X, Shu B, Zhang D, et al. The efficacy and safety of pharmacological treatments for post-stroke aphasia[J]. CNS Neurol Disord Drug Targets, 2018, 17(7): 509-21. doi: 10.2174/1871527317666180706143051 [12] Bocti C, Swartz RH, Gao FQ, et al. A new visual rating scale to assess strategic white matter hyperintensities within cholinergic pathways in dementia[J]. Stroke, 2005, 36(10): 2126-31. doi: 10.1161/01.STR.0000183615.07936.b6 [13] 高素荣, 王荫华. 失语症[M]. 北京: 北京医科大学、中国协和医科大学联合出版社, 1993: 1-37. [14] Mensing B, Nowak A, Zweifel S, et al. Morbus wilson oder hepatolentikuläre degeneration[J]. Ther Umschau, 2018, 75(4): 241-8. doi: 10.1024/0040-5930/a000995 [15] Smith KM, Caplan DN. Communication impairment in Parkinson's disease: Impact of motor and cognitive symptoms on speech and language[J]. Brain Lang, 2018, 185: 38-46. doi: 10.1016/j.bandl.2018.08.002 [16] Krishnan G, Tiwari S, Pai AR, et al. Variability in aphasia following subcortical hemorrhagic lesion[J]. Ann Neurosci, 2012, 19(4): 158-60. http://pubmedcentralcanada.ca/pmcc/articles/PMC4117060/ [17] Longworth CE, Keenan SE, Barker RA, et al. The basal Ganglia and rule-governed language use: evidence from vascular and degenerative conditions [J]. Brain, 2005, 128(Pt 3): 584-96. http://europepmc.org/abstract/med/15659423 [18] de Boissezon X, Démonet JF, Puel M, et al. Subcortical aphasia: a longitudinal PET study[J]. Stroke, 2005, 36(7): 1467-73. doi: 10.1161/01.STR.0000169947.08972.4f [19] De Boissezon X, Marie N, Castel-Lacanal E, et al. Good recovery from aphasia is also supported by right basal ganglia: a longitudinal controlled PET study. EJPRM-ESPRM 2008 award winner [J]. Eur J Phys Rehabil Med, 2009, 45(4): 547-58. http://europepmc.org/abstract/MED/20032914 [20] Katanoda K, Yoshikawa K, Sugishita M. A functional MRI study on the neural substrates for writing[J]. Hum Brain Mapp, 2001, 13(1): 34-42. doi: 10.1002/hbm.1023 [21] Hoover JE, Strick PL. Multiple output channels in the basal Ganglia [J]. Science, 1993, 259(5096): 819-21. doi: 10.1126/science.7679223 [22] Tettamanti M, Moro A, Messa C, et al. Basal Ganglia and language: phonology modulates dopaminergic release[J]. Neuroreport, 2005, 16(4): 397-401. doi: 10.1097/00001756-200503150-00018 [23] 毛善平, 陈卓铭, 李承晏, 等. 皮层下失语的语言特点及与病灶部位关系的研究[J]. 中国病理生理杂志, 2002, 18(8): 927-30. https://www.cnki.com.cn/Article/CJFDTOTAL-ZBLS200208014.htm [24] 刘晓加, 戴蓉, 邵明, 等. 基底节病变时语言障碍的书写特点[J]. 中国神经精神疾病杂志, 2006, 32(5): 418-22. https://www.cnki.com.cn/Article/CJFDTOTAL-ZSJJ200605009.htm [25] Dickey L, Kagan A, Lindsay MP, et al. Incidence and profile of inpatient stroke-induced aphasia in Ontario, Canada[J]. Arch Phys Med Rehabil, 2010, 91(2): 196-202. doi: 10.1016/j.apmr.2009.09.020 [26] Zhang C, Zhou P, Yuan T. The cholinergic system in the cerebellum: from structure to function[J]. Rev Neurosci, 2016, 27(8): 769-76. doi: 10.1515/revneuro-2016-0008 [27] Kumar M, Sandhir R. Hydrogen sulfide suppresses homocysteineinduced glial activation and inflammatory response[J]. Nitric Oxide, 2019, 90: 15-28. doi: 10.1016/j.niox.2019.05.008 [28] Ganguly P, Alam SF. Role of homocysteine in the development of cardiovascular disease[J]. Nutr J, 2015, 14: 6. doi: 10.1186/1475-2891-14-6 [29] Ji YF, Li XY, Teng ZJ, et al. Homocysteine is associated with the development of cerebral small vessel disease: retrospective analyses from neuroimaging and cognitive outcomes [J]. J Stroke Cerebrovasc Dis, 2020, 29(12): 105393. doi: 10.1016/j.jstrokecerebrovasdis.2020.105393 [30] Poddar R. Hyperhomocysteinemia is an emerging comorbidity in ischemic stroke[J]. Exp Neurol, 2021, 336: 113541. doi: 10.1016/j.expneurol.2020.113541 [31] Naka H, Nomura E, Takahashi T, et al. Plasma total homocysteine levels are associated with advanced leukoaraiosis but not with asymptomatic microbleeds on T2*-weighted MRI in patients with stroke[J]. Eur J Neurol, 2006, 13(3): 261-5. doi: 10.1111/j.1468-1331.2006.01205.x [32] Wright A, Tippett D, Saxena S, et al. Leukoaraiosis is independently associated with Naming outcome in poststroke aphasia [J]. Neurology, 2018, 91(6): e526-e532. doi: 10.1212/WNL.0000000000005945 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 459
- HTML全文浏览量: 161
- PDF下载量: 7
- 被引次数: 0