



Preoperative CT findings and their relationship with conversion to thoracotomy in patients undergoing video assisted thoracoscopic lobectomy
-
摘要:
目的研究术前CT指标与全胸腔镜(VATS)肺叶切除手术中转开胸之间的关系。 方法选取2016年12月~2019年12月我院871例肺部占位性病变患者为样本进行前瞻性研究,均完成CT检查并进行VATS肺叶切除术,其中中转开胸手术者为28例(3.21%),作为中转组; 采用随机数字表法从顺利完成VATS手术的患者中抽取100例作为VATS组,比较两组一般资料、CT检查结果及手术结果,分析术前CT检查对VATS中转开胸的影响和预测价值。 结果VATS组手术时间、术中出血量、引流时间及住院时间均低于中转组,差异有统计学意义(P < 0.05); 两组术后感染、气胸及肺不张等并发症差异无统计学意义(P>0.05); VATS组CT征象中最大淋巴结短径以及肿瘤浸润和胸膜凹陷征发生率均低于中转组(P < 0.05),两组肺野病灶位置、病灶最大径和淋巴结钙化比较差异无统计学意义(P>0.05); Logistics回归分析显示肿瘤浸润是影响VATS中转开胸的独立危险因素(P < 0.05); ROC曲线分析示肿瘤浸润、最大淋巴结短径、胸膜凹陷征以及3项CT指标联合预测VATS中转开胸的灵敏度分别为82.14%、67.86%、67.86%和78.57%,特异度分别为89.00%、69.00%、93.00%和93.00%。 结论VATS中转开胸可对患者术后康复造成不良影响,其主要原因为肿瘤浸润或淋巴结粘连导致血管等解剖结构分离难度增加,肿瘤浸润、最大淋巴结短径和胸膜凹陷征等术前CT指标对评估中转开胸风险具有一定参考价值。 Abstract:ObjectiveTo explore the relationship between the preoperative CT indexes and conversion to thoracotomy during video assisted thoracoscopic surgery (VATS) lobectomy. MethodsA total of 871 patients with lung space-occupying lesions in our hospital from December 2016 to December 2019 were selected. The patients completed the CT examination and underwent VATS lobectomy. Among them, 28 cases were converted to thoracotomy, accounting for 3.21%. 100 cases from patients who successfully completed VATS surgery were extracted as VATS group by the random number table method. The general data, CT examination results and surgical results were compared between the two groups. The influence and predictive value of preoperative CT examination on conversion of VATS to thoracotomy were analyzed. ResultsThe surgical time, intraoperative blood loss, drainage time and hospitalization timem in VATS group were significantly lower than those in conversion group(P < 0.05). There were no significant differences in the complications such as postoperative infection, pneumothorax and atelectasis between the two groups (P>0.05). The CT signs of short diameter of the largest lymph node and incidence rates of tumor infiltration and pleural indentation in VATS group were significantly lower than those in conversion group (P < 0.05). There were no significant differences in the location of lung field lesions, the largest diameter of lesions and lymph node calcification between the two groups (P>0.05). Logistics regression analysis showed that tumor infiltration was an independent risk factor affecting the conversion to thoracotomy in VATS (P < 0.05). ROC curve analysis showed that the sensitivities of tumor infiltration, short diameter of the largest lymph node, pleural indentation and the combination of the three CT indexes in predicting VATS conversion to thoracotomy were 82.14%, 67.86%, 67.86% and 78.57%, and the specificities were 89.00%, 69.00%, 93.00% and 93.00% respectively. ConclusionVATS conversion to thoracotomy can adversely affect postoperative rehabilitation of patients. The main reasons are that tumor infiltration or lymph node adhesion leads to increase difficulty in separating blood vessels and other anatomical structures, and preoperative CT indexes such as tumor infiltration, short diameter of the largest lymph node and pleural indentation have a certain reference value in assessing the risk of conversion to thoracotomy. -

图 1 男性NSCLC患者,62岁,术前CT检查显示左肺上叶占位性病变
A: 肺窗; B: 纵隔窗; C: 左肺动脉及上干.
Figure 1. A 62-year-old male patient with NSCLC, preoperative CT examination revealed upper lobe space-occupying lesions of the left lung.

图 2 女性NSCLC患者,57岁,术前CT检查显示左肺上叶肿瘤
A: 肺窗; B: 纵隔窗; C: 伴肺门淋巴结转移肿大压迫左肺动脉上干根部.
Figure 2. A57-year-old female patient with NSCLC, preoperative CT examination showed left lung upper lobe tumors.

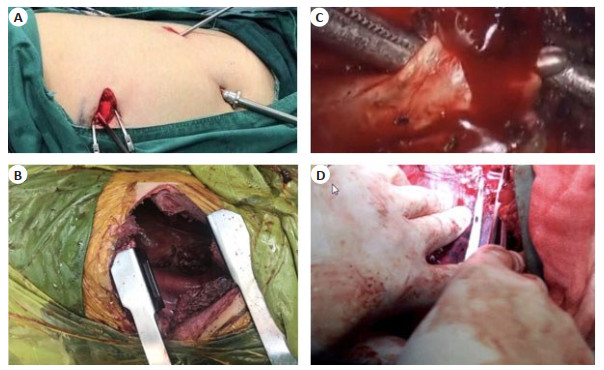
图 3 全胸腔镜肺叶切除手术中转开胸
A: 三孔胸腔镜切口; B: 胸腔镜中转开胸切口; C: 左肺动脉上干根部破裂出血; D: 中转开胸缝合止血.
Figure 3. VATS conversion to thoracotomy.
表 1 两组一般资料比较
Table 1. Comparison of general data between the two groups
分组 性別 年龄
(岁,Mean±SD)疾病类型 男 女 肺腺癌 肺鱗癌 支气管扩张 结核瘤 转移癌 其它 VATS组(n=100) 53 47 50.91±10.26 65 13 7 4 3 8 中转组(n=28) 15 13 51.48±10.79 22 4 0 1 0 1 t/χ2 0.003 0.257 - P 0.957 0.798 0.786 VATS: 全胸腔镜手术.  下载: 导出CSV
下载: 导出CSV
表 2 两组围术期指标比较
Table 2. Comparison of perioperative indexes between the two groups (Mean±SD)
分组 手术时间(min) 术中出血量(mL) 引流时间(d) 住院时间(d) VATS组(n=100) 183.65±49.23 274.38±65.49 5.96±1.27 10.85±2.73 中转组(n=28) 241.39±62.07 406.81±92.53 7.82±2.14 13.46±3.52 t 5.169 8.586 5.801 4.184 P < 0.001 < 0.001 < 0.001 < 0.001
下载: 导出CSV
表 3 两组术后并发症比较
Table 3. Comparison of postoperative complications between the two groups [n(%)]
分组 切口感染 肺部感染 气胸 肺不张 心律失常 VATS组(n=100) 4(4.00) 2(2.00) 6(6.00) 3(3.00) 4(4.00) 中转组(n=28) 3(10.71) 1(3.57) 2(7.14) 0(0) 2(7.14) χ2 1.908 - 0.049 - - P 0.167 0.526 0.825 1.000 0.611
下载: 导出CSV
表 4 两组CT征象比较
Table 4. Comparison of CT signs between the two groups
分组 肺野病灶位置[n(%)] 肿瘤浸润K%)] 病灶最大径(cm) 最大淋巴结短径(cm) 淋巴结钙化K%)] 胸膜凹陷征K%)] 外1/3 中1/3 内1/3 VATS组(n=100) 67 28 5 1(11.00) 2.81±0.54 0.89±0.25 6(6.00) 7(7.00) 中转组(n=28) 16 10 2 23(82.14) 3.01±0.62 1.07±0.31 4(14.29) 19(67.86) t/χ2 0.950 56.758 1.676 3.189 2.085 50.052 P 0.622 < 0.001 0.096 0.002 0.149 < 0.001
下载: 导出CSV
表 5 VATS中转开胸的危险因素分析
Table 5. Risk factors of VATS conversion to thoracotomy
相关因素 SE χ2 OR 95%CI P 肿瘤浸润 2.856 0.848 11.343 17.392 3.300~91.659 0.001 最大淋巴结短径 0.878 1.129 0.605 2.407 0.263~21.994 0.436 胸膜凹陷征 0.908 0.846 1.152 2.478 0.472~13.006 0.283 常量 -3.699 1.173 9.942 0.025 - 0.002
下载: 导出CSV
表 6 CT指标对VATS中转开胸预测价值分析
Table 6. Predictive value of CT indexes on VATS conversion to thoracotomy
DCE参数 AUC SE 95%CI 约登指数 灵敏度(%) 特异度(%) 肿瘤浸润 0.856 0.040 0.783~0.912 0.711 82.14 89.00 最大淋巴结短径 0.650 0.068 0.561~0.732 0.369 67.86 69.00 胸膜凹陷征 0.804 0.047 0.725~0.869 0.609 67.86 93.00 联合预测 0.855 0.054 0.781~0.911 0.716 78.57 93.00
下载: 导出CSV
-
[1] Dumitra TC, Molina JC, Mouhanna J, et al. Feasibility analysis for the development of a video-assisted thoracoscopic (VATS) lobectomy 23-hour recovery pathway[J]. Can J Surg, 2020: E349- 58. doi: 10.1503/cjs.002219 [2] Umari M, Falini S, Segat M, et al. Anesthesia and fast-track in videoassisted thoracic surgery (VATS): from evidence to practice[J]. J Thorac Dis, 2018, 10(suppl 4): S542-54. http://www.ncbi.nlm.nih.gov/pubmed/29629201 [3] Amore D, Imitazione P, Palma A, et al. Conversion to thoracotomy during VATS segmentectomy for treatment of symptomatic endobronchial hamartoma[J]. Int J Surg Case Rep, 2018, 51: 272-4. doi: 10.1016/j.ijscr.2018.09.006 [4] 黄小龙, 杨柳山, 吴西林. 全胸腔镜肺癌切除术中转开胸原因分析[J]. 临床外科杂志, 2016(9): 712-3. https://www.cnki.com.cn/Article/CJFDTOTAL-LCWK201609028.htm [5] Augustin F, Maier HT, Weissenbacher A, et al. Causes, predictors and consequences of conversion from VATS to open lung lobectomy [J]. Surg Endosc, 2016, 30(6): 2415-21. doi: 10.1007/s00464-015-4492-3 [6] 李海, 徐刚, 宋永祥, 等. 非小细胞肺癌患者电视辅助胸腔镜肺叶切除术中转开胸的影响因素分析[J]. 安徽医科大学学报, 2018, 53(5): 809-11. https://www.cnki.com.cn/Article/CJFDTOTAL-YIKE201805032.htm [7] Bongiolatti S, Gonfiotti A, Viggiano D, et al. Risk factors and impact of conversion from VATS to open lobectomy: analysis from a national database[J]. Surg Endosc, 2019, 33(12): 3953-62. doi: 10.1007/s00464-019-06682-5 [8] Park SC, Tan J, Wang XW, et al. Computer-aided detection of early interstitial lung diseases using low-dose CT images[J]. Phys Med Biol, 2011, 56(4): 1139-53. doi: 10.1088/0031-9155/56/4/016 [9] Watanabe R, Funama Y, Takaki T, et al. Additive value of split-bolus single-phase CT scan protocol for preoperative assessment of lung cancer patients referred for video-assisted thoracic surgery[J]. Radiol Phys Technol, 2019, 12(4): 409-16. doi: 10.1007/s12194-019-00541-7 [10] 陈楠, 丁莹莹, 廖承德, 等. 术前CT指标对全胸腔镜肺叶切除手术中转开胸的预测价值[J]. 昆明医科大学学报, 2019, 40(6): 93-7. https://www.cnki.com.cn/Article/CJFDTOTAL-KMYX201906020.htm [11] 宋小运, 韩毅, 苏崇玉, 等. 单手术组全胸腔镜支气管袖式肺叶切除术与开胸手术近期疗效对比[J]. 实用医学杂志, 2016, 32(16): 2716-8. https://www.cnki.com.cn/Article/CJFDTOTAL-SYYZ201616040.htm [12] 叶敬霆, 孙超, 陆世春, 等. 电视胸腔镜手术在肺结节诊治中的研究进展[J]. 中华胸部外科电子杂志, 2018, 5(2): 118-23. https://www.cnki.com.cn/Article/CJFDTOTAL-XBWK201802010.htm [13] 田明发. 全胸腔镜肺叶切除术与传统开胸手术治疗早期非小细胞肺癌的疗效研究[J]. 中国处方药, 2018, 16(4): 50-1. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGCF201804034.htm [14] Li SJ, Zhou K, Wu YM, et al. Presence of pleural adhesions can predict conversion to thoracotomy and postoperative surgical complications in patients undergoing video-assisted thoracoscopic lung cancer lobectomy[J]. J Thorac Dis, 2018, 10(1): 416-31. doi: 10.21037/jtd.2017.12.70 [15] Amore D, di Natale D, Scaramuzzi R, et al. Reasons for conversion during VATS lobectomy: what happens with increased experience [J]. J Vis Surg, 2018, 4: 53. doi: 10.21037/jovs.2018.03.02 [16] 李华伟, 王海艳, 张临友. 肺癌患者胸腔镜下肺叶切除术中转开胸危险因素分析[J]. 中国胸心血管外科临床杂志, 2017, 24(12): 962-9. https://www.cnki.com.cn/Article/CJFDTOTAL-ZXYX201712012.htm [17] Li Y, Wang J. Analysis of lymph node impact on conversion of complete thoracoscopic lobectomy to open thoracotomy[J]. Thorac Cancer, 2015, 6(6): 704-8. doi: 10.1111/1759-7714.12241 [18] 李运, 杨帆, 赵辉, 等. 全胸腔镜肺叶切除术中转开胸的淋巴结影响[J]. 中华胸心血管外科杂志, 2013, 29(10): 591-4. [19] 邱小琴, 黄凯, 吴诏周, 等. 多导螺旋CT后处理技术多平面重组及最小密度投影诊断支气管扩张的价值[J]. 分子影像学杂志, 2019, 42 (2): 160-5. doi: 10.12122/j.issn.1674-4500.2019.02.04 [20] Digumarthy SR, Padole AM, Lo Gullo R, et al. CT texture analysis of histologically proven benign and malignant lung lesions[J]. Medicine, 2018, 97(26): e11172. http://www.ncbi.nlm.nih.gov/pubmed/29952966 [21] Guo CL, Mei JD, Liu CW, et al. Video- assisted thoracic surgery compared with posterolateral thoracotomy for mediastinal bronchogenic cysts in adult patients[J]. J Thorac Dis, 2016, 8(9): 2504-11. doi: 10.21037/jtd.2016.08.29 -


 点击查看大图
点击查看大图

计量
- 文章访问数: 642
- HTML全文浏览量: 381
- PDF下载量: 4
- 被引次数: 0