



Clinical value of laparoscopic single-site surgery for benign ovarian tumors and the prognostic value of combination of HE4, CA125 and β-HCG
-
摘要:
目的探讨血清人附睾蛋白4(HE4)、血清糖类抗原125(CA125)及人绒毛膜促性腺激素(β-HCG)水平联合预测经脐单孔腹腔镜手术治疗卵巢良性肿瘤疗效的临床价值。 方法回顾分析2017年1月~2019年3月于我院妇产科确诊为卵巢良性肿瘤的120例患者,依据患者选择手术方式的不同分为两组:观察组选择单孔腹腔镜手术治疗,共72例,年龄21~63岁(32.98±9.34岁),肿瘤直径3.69~9.78 cm(5.46±3.65 cm);对照组选择传统多孔腹腔镜手术治疗,共48例,年龄19~68岁(33.02±9.35岁),肿瘤直径3.82~9.93 cm(5.61±3.68 cm)。检测两组血清HE4、CA125及β-HCG水平,并观察两组疗效,进行比较分析。 结果两组患者手术过程顺利,无术中与术后并发症。观察组与对照组比较,术中出血情况、排气时间差异无统计学意义(P>0.05);观察组的手术时间比对照组长(P<0.05),但观察组的住院时间较对照组短(P<0.05),且患者满意度评分均高于对照组(P<0.05)。两组术前血清HE4、CA125及β-HCG水平比较差异无统计学意义(P>0.05),两组术后血清HE4、CA125及β-HCG水平较术前降低,差异有统计学意义(P<0.05)。观察组术后12 h的HE4、CA125及β-HCG水平比术后1、3 d降低(P<0.05),术后1、3 d之间差异无统计学意义(P>0.05);对照组术后12 h、1 d、3 d差异均有统计学意义(P<0.05)。ROC分析显示,HE4、CA125、β-HCG的曲线下面积分别为:0.901、0.820、0.736;各项指标联合检测的曲线下面积为0.957。 结论血清HE4、CA125及β-HCG水平联合检测可有效评价单孔腹腔镜手术治疗卵巢良性肿瘤的临床疗效,且达到预期疗效的同时,提高了患者满意度,值得临床推广。 Abstract:ObjectiveTo investigate the clinical value of serum human epididymis protein 4 (HE4), serum carbohydrate antigen 125(CA125), and β-Human chorionic gonadotropin(β-HCG)levels in combination to predict the efficacy of laparoscopic single-site surgery in the treatment of benign ovarian tumor. MethodsFrom January 2017 to March 2019, 120 cases of benign ovarian tumors were diagnosed after treatment in the department of obstetrics and gynecology of our hospital. The patients were divided into two groups according to different surgical methods. The observation group chosed single-hole laparoscopic surgery for 72 patients, with the age from 21 to 63 years old (average 32.98±9.34) and the tumor diameter from 3.69~9.78 cm (average 5.46±3.65 cm), while the control group chosed traditional multi-site laparoscopic surgery for 48 patients, with the age from 19 to 68 years old (average 33.02±9.35) and the tumor diameter from 3.82 to 9.93 cm (average 5.61±3.68 cm). Serum levels of HE4, CA125 and β-HCG in the two groups were detected, and the effects of the two groups was observed for comparative analysis. ResultsThe operation of the two groups was smooth, without intraoperative or postoperative complications. The difference in intraoperative bleeding and exhaust time between the observation group and the control group was not significant (P>0.05). The operation time of the observation group was longer than that of the control group (P<0.05). The length of time of the observation group was shorter than that of the control group (P<0.05), and the patient satisfaction score was higher than that of the control group (P<0.05). The difference in serum HE4, CA125 and β-HCG between the two groups before surgery was not significant (P>0.05). The postoperative serum HE4, CA125 and β-HCG between the two groups were significantly lower than those before surgery (P<0.05). The levels of HE4, CA125 and β-HCG in the observation group at 12 hours after the operation were significantly lower than those at 1 day and 3 days after the operation (P<0.05). The difference between 1 day and 3 days after the operation was not significant(P>0.05). The differences in the control group at 12 hours, 1 day and 3 days after surgery were significant(P<0.05). ROC analysis showed that the AUC of all indexes were: HE4 (0.901), CA125 (0.820) and β-HCG(0.736), AUC of all indexes was 0.957. ConclusionThe combined detection of serum HE4, CA125 and β-HCG levels can effectively evaluate the clinical efficacy of laparoscopic single-site surgery in the treatment of benign ovarian tumors. It can achieve the expected efficacy and improve patient satisfaction. -

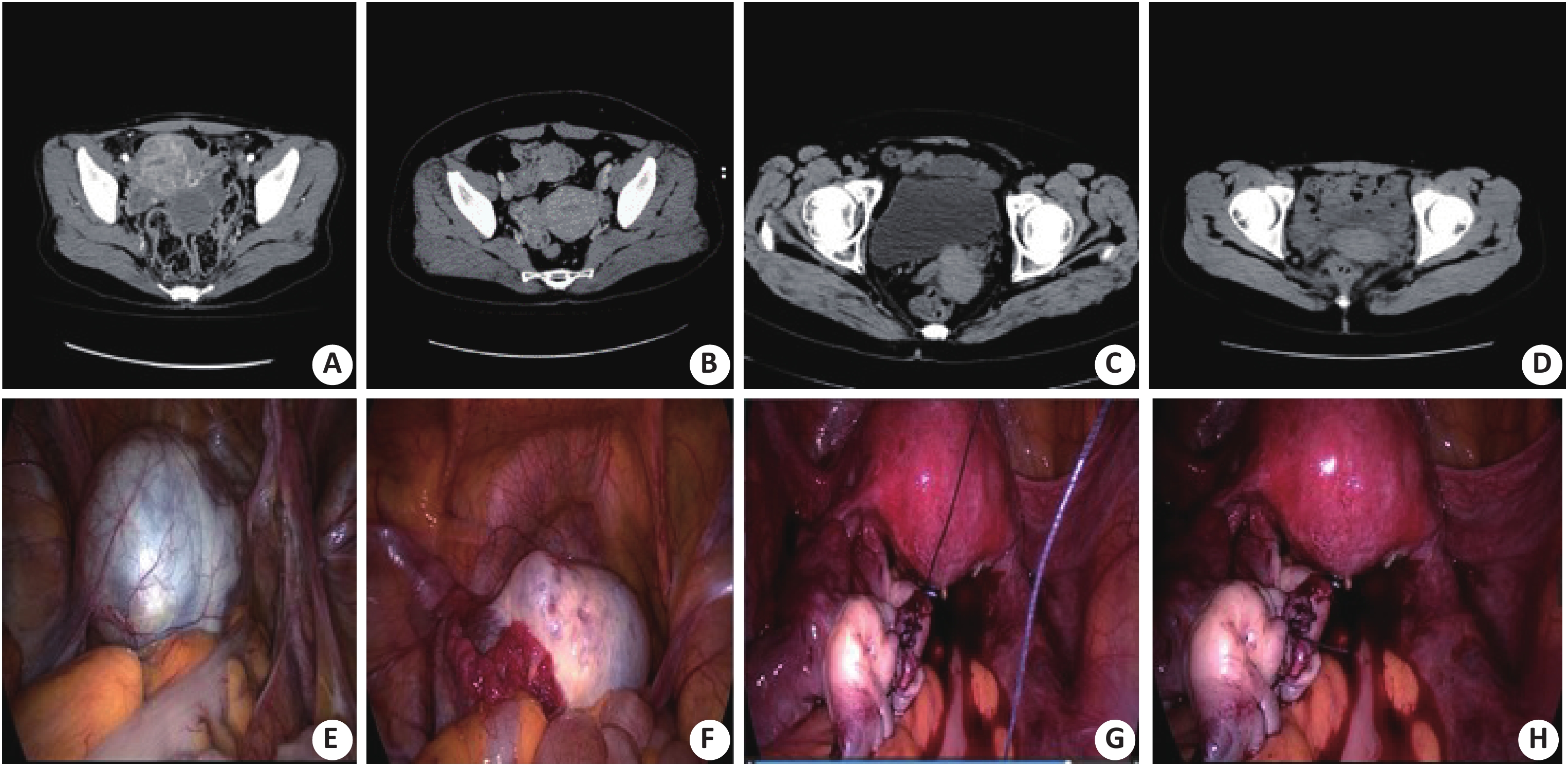
图 1 两组术前、术后CT及并发症情况
A:观察组术前;B:对照组术前;C:观察组术后;D:对照组术后;E:术中切除前情况;F:术中切除剥离肿瘤过程;G:术中肿瘤切除情况;H:术中切除后情况;A-D为CT增强影像,E-H为腹腔镜下观察图.
Figure 1. CT and complications before and after operation in two groups
表 1 两组临床疗效的比较(Mean±SD)
Table 1. Comparison of clinical efficacy between two groups
类目 术中出血量(mL) 术后排气时间(h) 手术时间(min) 术后住院时间(d) 患者满意度评分(分) 观察组(n=72) 18.02±7.98 10.49±2.57 68.52±15.38 2.21±1.03 4.70±0.92 对照组(n=48) 27.75±11.46 15.89±3.09 53.91±12.87 4.38±1.84 3.65±0.58 t 4.170 4.961 2.653 3.493 6.641 P 0.006 0.004 0.033 0.008 0.000  下载: 导出CSV
下载: 导出CSV
表 2 两组HE4、CA125及β-HCG水平的比较(Mean±SD)
Table 2. Comparison of HE4、CA125 and β-HCG levels between two groups
指标 组别 术前 术后12 h 术后第1天 术后第3天 HE4(pmol/L) 观察组(n=72) 272.02±29.98# 68.18±9.23*a 43.67±4.15* 45.01±4.54 对照组(n=48) 269.91±29.83# 145.43±18.01a 98.57±11.02 46.83±4.56 CA125(U/mL) 观察组(n=72) 106.23±13.46# 47.86±4.09*a 30.99±3.17* 31.70±3.18 对照组(n=48) 104.79±13.42# 76.71±9.79a 52.84±4.80b 31.98±3.19 β-HCG(mU/mL) 观察组(n=72) 19.88±10.30# 5.94±2.06*a 2.95±1.73* 3.01±1.74 对照组(n=48) 19.64±10.29# 10.42±6.67a 6.97±2.73 3.25±1.79 *P<0.05 vs对照组; #P<0.05 vs术后12 h、1 d、3 d;aP<0.05vs术后1 d、3 d.
下载: 导出CSV
表 3 HE4、CA125及β-HCG单独与联合检测诊断卵巢良性肿瘤的价值
Table 3. Value of HE4、CA125 and β-HCG alone and in combination for diagnosis of benign ovarian tumors
类目 AUC 标准误 P 渐进95%置信区间 HE4 0.901 0.028 0.000 0.853-0.969 CA125 0.820 0.047 0.000 0.711-0.914 β-HCG 0.736 0.053 0.002 0.627-0.835 三者联合 0.957 0.0207 0.000 0.916-0.984
下载: 导出CSV
-
[1] 吴金萍, 王志芳. 腹腔镜手术治疗卵巢良性肿瘤对机体免疫功能卵巢功能的影响[J]. 山西医药杂志, 2019, 48(23): 2953-5. doi: 10.3969/j.issn.0253-9926.2019.23.043 [2] Lang SM, Mills AM, Cantrell LA. Malignant brenner tumor of the ovary: review and case report[J]. Gynecol Oncol Rep, 2017, 6(3): 26-31. [3] Badiglian FL, Oshima CT, De OL, et al. Canonical and noncanonical Wnt pathway: a comparison among normal ovary, benign ovarian tumor and ovarian cancer[J]. Oncol Rep, 2009, 21(2): 313-20. [4] Agaba EA, Rainville H, Ikedilo O, et al. Incidence of port-site incisional hernia after single-incision laparoscopic surgery[J]. J Soc Laparoendosc Surg, 2014, 18(2): 204-10. doi: 10.4293/108680813X13693422518317 [5] Tranchart H, Ketoff S, Lainas P, et al. Single incision laparoscopic cholecystectomy: for what benefit[J]. HPB(Oxford), 2013, 15(6): 433-8. [6] Liu X, Wen MK, Liu HY, et al. Clinical retrospective control study of single-port laparoendoscopic and multi-port laparoscopic ovarian cystectomy[J]. Chin J Obstetr Gynecol, 2017, 52(10): 675-8. [7] Marocco, Francesco, Fanfani, et al. Laparoendoscopic single-site surgery for fertility-sparing staging of border line ovarian tumors: initial experience[J]. Surg Laparosc Endosc Percutan Tech, 2010, 20(5): e172-5. doi: 10.1097/SLE.0b013e3181f271ec [8] 苏红梅, 王 冬, 史华山, 等. 血清CA125、HE4及FS水平联合检测评价单孔腹腔镜手术治疗卵巢良性肿瘤疗效的临床价值分析[J]. 临床合理用药杂志, 2016, 9(1): 144-5. [9] Huang W, Zhu J. Effect of surgical treatment for ovarian benign neoplasms on ovarian reserve[J]. Reprod Contracept, 2012, 32(11): 771-6. [10] 肖 淑, 郑新秋, 欧海蔚, 等. 腹腔镜与开腹手术治疗老年良性卵巢肿瘤对患者免疫功能及神经内分泌功能的影响[J]. 海南医学院学报, 2016, 22(1): 62-5. [11] Fagotti A, Fanfani F, Marocco F, et al. Laparoendoscopic single-site surgery for the treatment of benign adnexal diseases: a pilot study[J]. Surg Endosc, 2011, 25(4): 1215-21. doi: 10.1007/s00464-010-1346-x [12] Liang W, Li J, Zhang W, et al. Prolonged postoperative ileus in gastric surgery: Is there any difference between laparoscopic and open surgery[J]. Cancer Med, 2019, 8(12): 5515-23. doi: 10.1002/cam4.2459 [13] 刘 辉, 佐满珍. 单孔腹腔镜在卵巢良性肿瘤等妇科疾病的应用[J]. 世界最新医学信息文摘, 2019, 19(92): 126-7. [14] 白敦红, 向 敏. 腹腔镜手术治疗妊娠期卵巢良性肿瘤的疗效及对孕妇术后妊娠结局及子代短期预后的影响[J]. 实用癌症杂志, 2019, 34(12): 2078-81, 2085. [15] Matsuhashi T, Matsui R, Hasegawa C, et al. Laparoscopic excision of a uterine adenomatoid tumor and a coexisting ovarian teratoma: a case report and literature review[J]. J Nippon Med Sch, 2017, 84(3): 139-43. doi: 10.1272/jnms.84.139 [16] Collins B, Corey SJ. Mature ovarian teratoma after treatment for unilateral retinoblastoma with nonmutated RB1[J]. J Pediatr Hematol Oncol, 2017, 39(6): 485-6. [17] 林丽淑, 任 溪, 陈 睿, 等. CA125、HE4、β-HCG和AMH联合检测在卵巢癌早期诊断中的应用价值[J]. 国际检验医学杂志, 2019, 40(13): 1553-6. doi: 10.3969/j.issn.1673-4130.2019.13.005 [18] Scaletta G, Plotti F, Luvero D, et al. The role of novel biomarker HE4 in the diagnosis, prognosis and follow-up of ovarian cancer: a systematic review[J]. Expert Rev Anticanc, 2017, 17(9): 827-39. doi: 10.1080/14737140.2017.1360138 [19] Wu RT, Tomg PL, Chang DY, et al. Mature cystic teratoma of the ovary: a clinicopathologic study of 283 cases[J]. Chin Med J (Taipei), 1996, 58(4): 269-74. [20] Emsal PT, Kumtepe Y. Endometrial and ovarian cancer with MR imaging importance of serum HE4 and CA 125 levels in the extent of disease at evaluation[J]. Eurasian J Med, 2017, 48(3): 192-8. doi: 10.5152/eurasianjmed.2016.0259 [21] Hasanbegovic L, Sljivo N. Determination of the reference values of the tumor marker HE4 in female population of canton sarajevo[J]. Mater Sociomed, 2018, 30(1): 15-9. doi: 10.5455/msm.2018.30.15-19 [22] 吴 音. 超声造影结合CA125在卵巢肿瘤鉴别诊断中的应用研究[C]. 中国超声医学工程学会. 中国超声医学工程学会第十届全国超声治疗及生物效应医学学术大会论文汇编. 中国超声医学工程学会: 中国超声医学工程学会, 2019: 59. [23] 左菲菲. 血清CA125检测在诊断卵巢良恶性肿瘤中的价值[J]. 包头医学院学报, 2015, 31(12): 71-3. [24] 熊 雯, 周新娥, 黄 娟, 等. 血清CA125、HE4及IL-17检测对上皮性卵巢癌的早期诊断价值分析[J]. 中国计划生育和妇产科, 2016, 8(3): 69-73. doi: 10.3969/j.issn.1674-4020.2016.03.20 [25] Braicu E, Van Gorp T, Nassir M, et al. Preoperative HE4 and ROMA values do not improve the CA125 diagnostic value for borderline tumors of the ovary (BOT)– a study of the TOC Consortium[J]. J Ovarian Res, 2014, 7(1): 49-5. doi: 10.1186/1757-2215-7-49 [26] Buamah PK, Cornell C, Skillen AW, et al. Initial assessment of tumor-associated antigen CA-125 in patients with ovarian, cervical, and testicular tumors[J]. Clin Chem, 1987, 33(7): 1124-5. doi: 10.1093/clinchem/33.7.1124 [27] Azahara PM, José MC, Madel PT. Value of [18F]FDG-PET/CT and CA125, serum levels and kinetic parameters, in early detection of ovarian cancer recurrence: Influence of histological subtypes and tumor stages[J]. Medicine, 2018, 97(17): e0098-105. doi: 10.1097/MD.0000000000010098 [28] 柳 洲, 颜 彦, 刘大庆, 等. 联合检测HE4与OPN及CA125对卵巢癌诊断价值的探讨[J]. 中华肿瘤防治杂志, 2012, 19(11): 856-9. [29] Bastani A, Asghary A, Heidari MH, et al. Evaluation of the sensitivity and specificity of serum level of prostasin, CA125, LDH, AFP, and hCG+β in epithelial ovarian cancer patients[J]. Eur J Gynaecol Oncol, 2017, 38(3): 418-24. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 771
- HTML全文浏览量: 266
- PDF下载量: 5
- 被引次数: 0