



Value of 18F-FDG PET/CT imaging combined with CA125 and HE4 in postoperative recurrence / metastasis of epithelial ovarian cancer
-
摘要:
目的探讨18F-脱氧葡萄糖PET/CT显像联合血清糖类抗原125及人附睾蛋白4检测在上皮性卵巢癌患者术后复发/转移中的诊断价值。 方法回顾性分析2018年7月~2019年9月在我院核医学科行18F-FDG PET/CT显像并显像前已行血清CA125及HE4值检测的65例上皮性卵巢癌患者作为研究对象。分18F-FDG PET/CT显像诊断组和18F-FDG PET/CT+CA125+HE4诊断组进行诊断并依据随访标准进行随访,各组诊断结果与随访结果进行比较。 结果18F-FDG PET/CT显像在评估上皮性卵巢癌患者术后复发/转移的灵敏度、特异度、阳性预测值、阴性预测值、一致率分别为96.22%、66.7%、92.73%、80.0%、90.77%。18F-FDG PET/CT+CA125+HE4评估上皮性卵巢癌患者术后复发/转移的灵敏度、特异度、阳性预测值、阴性预测值、一致率分别为98.1%、66.7%、92.9%、88.9%、92.3%。复发/转移组CA125及HE4受试者工作特征曲线得知临界值分别为20.65 U/mL、45.5 pmol/L。18F-FDG PET/CT+CA125临界值+HE4临界值评估上皮性卵巢癌患者术后复发/转移的灵敏度、特异度、阳性预测值、阴性预测值、一致率分别为98.1%、75.0%、94.6%、90.0%、93.9%。 结论18F-FDG PET/CT显像在评估上皮性卵巢癌患者术后复发/转移上有优势。18F-FDG PET/CT+CA125+HE4检测在评估上皮性卵巢癌患者术后复发/转移上有较高的诊断价值,三者联合检测优于单独检测及两者联合检测。18F-FDG PET/CT+CA125临界值+HE4临界值检测在评估上皮性卵巢癌患者术后复发/转移上有更高的诊断价值。在临床随访过程中发现血清CA125≥20.65 U/mL,血清HE4≥45.5 pmol/L,并持续增加时应保持警惕,并选择18F-FDG PET/CT显像来提高上皮性卵巢癌复发/转移检出率,早期发现复发/转移病灶。。 Abstract:ObjectiveTo investigate the diagnostic value of 18F-fluorodeoxyglucose PET/CT imaging combined with serum carbohydrate antigen 125 (CA125) and human epididymal protein 4 (HE4) in the diagnosis of postoperative recurrence / metastasis in patients with epithelial ovarian cancer. MethodsFrom July 2018 to September 2019, 65 patients with epithelial ovarian cancer who had detected serum CA125 and HE4 before 18F-FDG PET/CT imaging were retrospectively analyzed. The patients were divided into 18F-FDG PET/CT imaging diagnosis group and 18F-FDG PET/CT+CA125+HE4 diagnosis group and followed up according to the follow-up criteria. The diagnostic results of each group were compared with the follow-up results. ResultsThe sensitivity, specificity, positive predictive value, negative predictive value and consistent rate of 18F-FDG PET/CT imaging in evaluating postoperative recurrence / metastasis of patients with epithelial ovarian cancer were 96.22%, 66.7%, 92.73%, 80.0%, 90.77%, respectively. The sensitivity, specificity, positive predictive value, negative predictive value and consistent rate of 18F-FDG PET/CT+CA125+HE4 in evaluating postoperative recurrence / metastasis of patients with epithelial ovarian cancer were 98.1%, 66.7%, 92.9%, 88.9% and 92.3%, respectively. Receiver operating characteristic of CA125 and HE4 subjects in recurrence / metastasis group showed that the critical value were 20.65 U/mL and 45.5 pmol/L respectively. The sensitivity, specificity, positive predictive value, negative predictive value and consistent rate of 18F-FDG PET/CT+CA125critical value + HE4critical value for evaluating postoperative recurrence / metastasis of epithelial ovarian cancer patients were 98.1%, 75.0%, 94.6%, 90.0%, 93.9%, respectively. Conclusion18F-FDG PET/CT imaging has an advantage in evaluating postoperative recurrence / metastasis in patients with epithelial ovarian cancer. 18F-FDG PET/CT+CA125+HE4 detection has a high diagnostic value in evaluating postoperative recurrence / metastasis in patients with epithelial ovarian cancer. The combined detection of the three is better than that of single detection and combined detection of both. The detection of 18F-FDG PET/CT+CA125critical value + HE4critical value has a higher diagnostic value in evaluating postoperative recurrence/metastasis of patients with epithelial ovarian cancer. During the clinical follow-up, it was found that serum CA125≥20.65 U/mL and serum HE4≥45.5 pmol/L. We should be vigilant when it continues to increase, and 18F-FDG PET/CT imaging should be selected to improve the detection rate of recurrence/metastasis of epithelial ovarian cancer and to detect recurrence/metastasis lesions in the early stage. -
Key words:
- ovarian cancer /
- PET / CT imaging /
- CA125 /
- HE4 /
- recurrence /
- metastasis
-

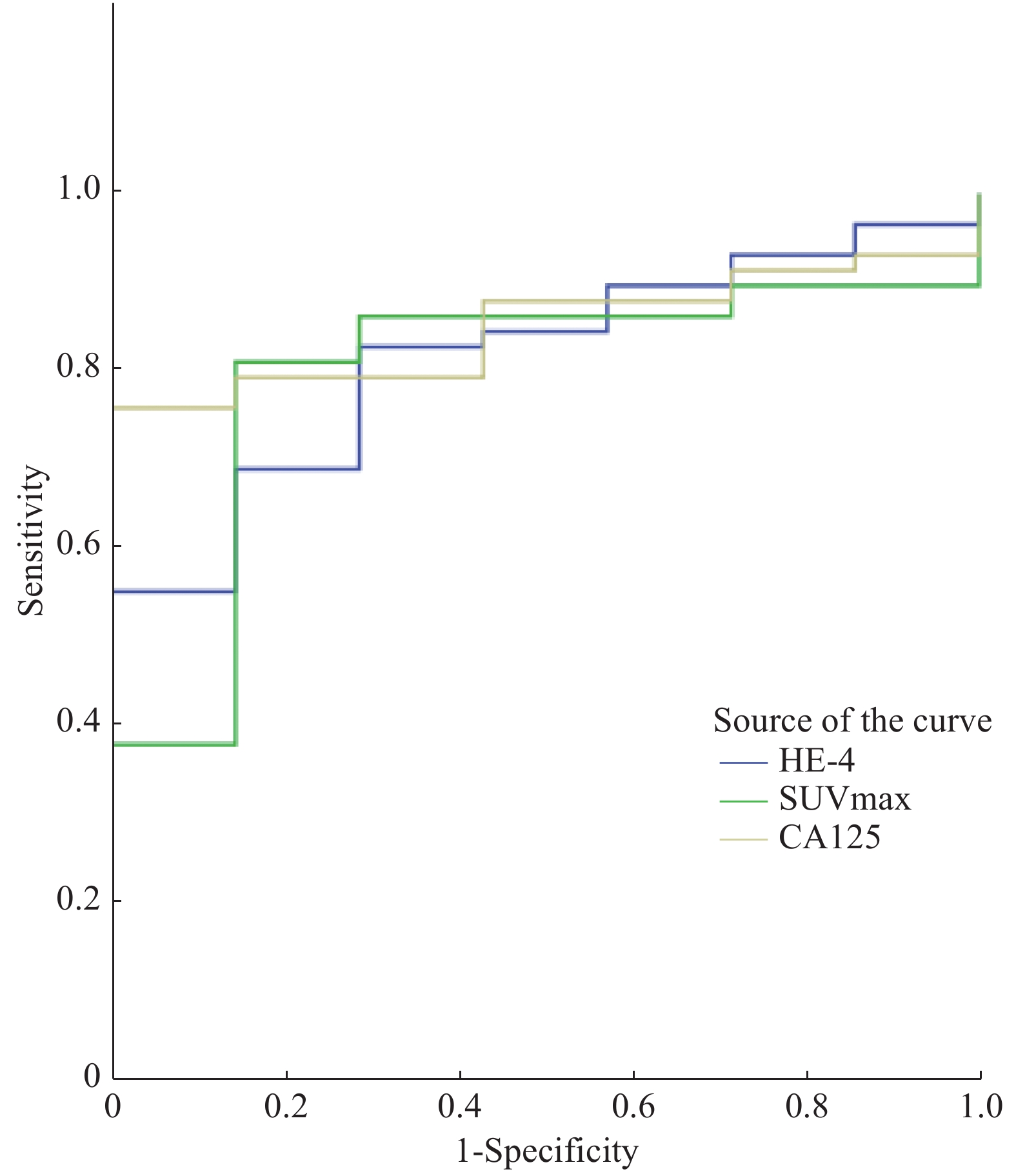
图 1 复发,转移组SUVmax,CA125及HE4诊断效能ROC曲线
Figure 1. ROC curves of SUVmax, CA125 and HE4 diagnostic efficacy of recurrence and metastasis

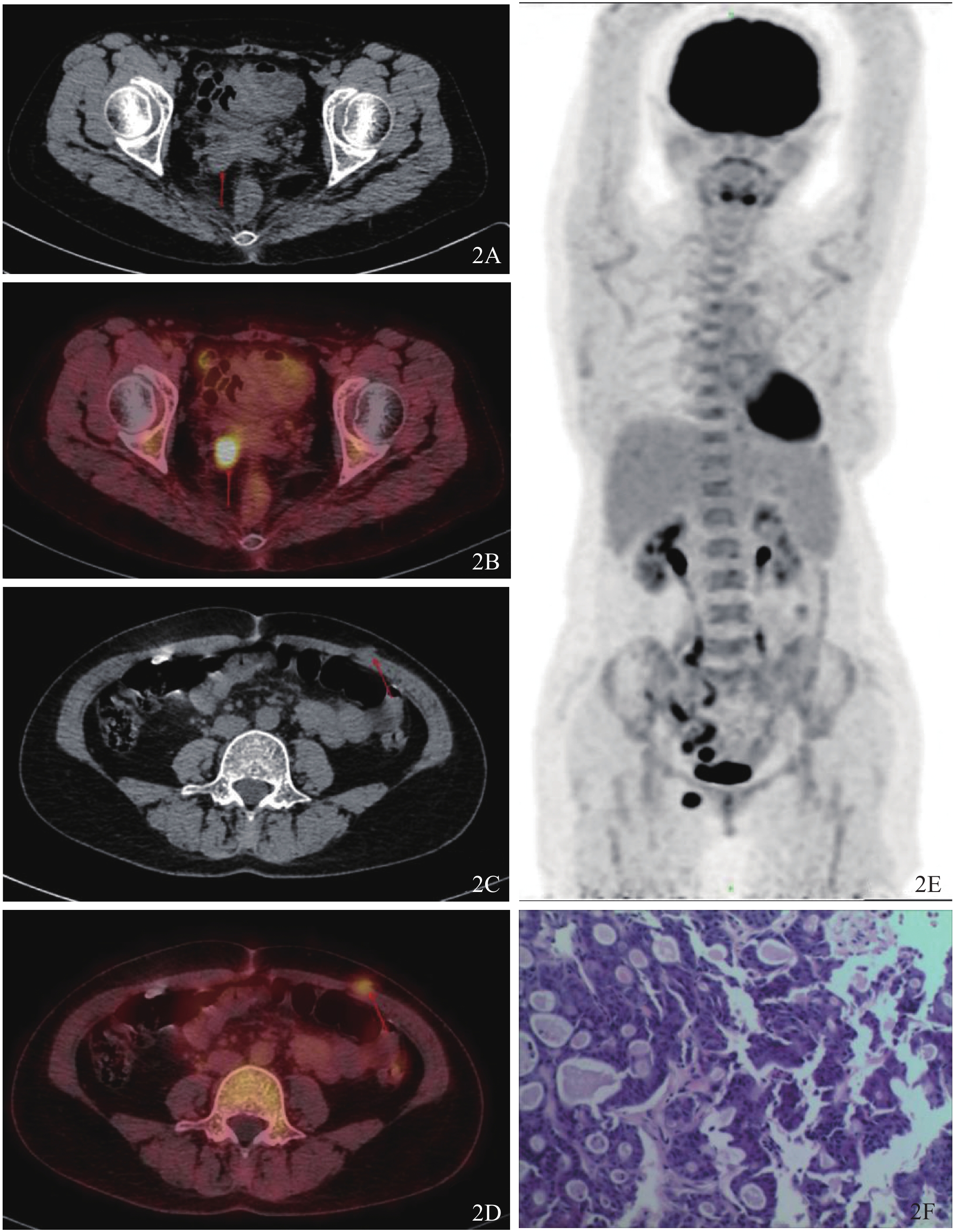
图 2 18F-FDG PET/CT显像及病理结果图
患者52岁,术前已绝经(46岁绝经),病理类型为子宫内膜样癌(低分化),初诊分期为IIB期. 血清CA125为8.50 U/mL,血清HE4为38.9 pmol/L. 18F-FDG PET/CT显像结果提示:阴道残端两侧结节伴FDG代谢活跃,考虑转移瘤,大小分别为2.4 cm×2.2 cm(A、B),SUVmax约5.76(右侧);2.4 cm×2.1 cm,SUVmax约2.17(左侧);左侧下腹壁结节伴FDG代谢活跃,考虑转移瘤,大小约1.5×1.0 cm(C、D),SUVmax约14.2. E:下腹部及盆腔腹膜I级增厚;F:腹壁肿物穿刺病理结果为腺癌.
Figure 2. 18F-FDG PET/CT imaging and pathological findings
表 1 18F-FDG PET/CT显像检测结果与随访结果的比较(n)
Table 1. Comparison between 18F-FDG PET/CT imaging and follow-up result
诊断方法 随访结果 合计 阳性 阴性 PET/CT 阳性 51 4 55 阴性 2 8 10 合计 53 12 65  下载: 导出CSV
下载: 导出CSV
表 2 联合检测诊断结果(%)
Table 2. Diagnostic result of combined detection
诊断方式 灵敏度 特异度 阳性预测值 阴性预测值 一致率 PET/CT+CA125 94.3 66.7 92.6 72.7 89.2 PET/CT+HE4 92.5 66.7 92.5 66.7 87.7 PET/CT+CA125+HE4 98.1 66.7 92.9 88.9 78.2
下载: 导出CSV
表 3 PET/CT+CA125临界值+HE4临界值检测结果(%)
Table 3. Result of PET/CT+CA125critical value + HE4critical value
诊断方式 灵敏度 特异度 阳性预测值 阴性预测值 一致率 PET/CT+CA125临界值+
HE4临界值98.1 75.0 94.6 90.0 93.9
下载: 导出CSV
-
[1] Torre LA, Bray F, Siegel RL, et al. Global cancer statistics, 2012[J]. Cancer J Clin, 2015, 65(2): 87-108. doi: 10.3322/caac.21262 [2] Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2009[J]. Cancer J Clin, 2010, 59(4): 225-49. [3] Berek JS, Crum C, Friedlander M. Cancer of the ovary, fallopian tube, and peritoneum[J]. Int J Gynaecol Obstet, 2015, 131(Suppl 2): S111-22. [4] Ledermann JA, Raja FA, Fotopoulou C, et al. Newly diagnosed and relapsed epithelial ovarian carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up[J]. Ann Oncol, 2013, 24(6): vi24-32. [5] Steffensen KD, Waldstrøm M, Brandslund I, et al. Prognostic impact of prechemotherapy serum levels of HER2, CA125, and HE4 in ovarian cancer patients[J]. Intern J Gynecolog Cancer, 2011, 21(6): 1040-51. doi: 10.1097/IGC.0b013e31821e052e [6] Zhang P, Wang C, Cheng L, et al. Comparison of HE4, CA125, and ROMA diagnostic accuracy: a prospective and multicenter study for Chinese women with epithelial ovarian cancer[J]. Medicine (Baltimore), 2015, 94(52): e240-51. [7] Hellström I, Raycraft J, Haydenledbetter M, et al. The HE4(WFDC2) Protein is a biomarker for ovarian carcinoma[J]. Cancer Res, 2003, 63(13): 3695-9. [8] Sironi S, Messa C, Mangili G, et al. Integrated FDG PET/CT in patients with persistent ovarian cancer: correlation with histologic findings[J]. Radiology, 2004, 233(2): 433-40. doi: 10.1148/radiol.2332031800 [9] 卢淮武, 林仲秋. 《2018 NCCN卵巢癌包括输卵管癌及原发性腹膜癌临床实践指南》解读[J]. 中国实用妇科与产科杂志, 2018, 34(5): 66-76. [10] 卢淮武, 霍楚莹, 林仲秋. 《2019NCCN卵巢癌包括输卵管癌及原发性腹膜癌临床实践指南(第1版)》解读[J]. 中国实用妇科与产科杂志, 2019, 35(5): 52-62. [11] Prat J. Ovarian carcinomas: fifive distinct diseases with different origins, genetic alterations, and clinicopathological features[J]. Virchows Arch, 2012, 460(3): 237-49. doi: 10.1007/s00428-012-1203-5 [12] Rusu D, Carlier T, Colombié M, et al. Clinical and survival im-pact of FDG PET in patients with suspicion of recurrent ovarian can-cer: a 6-year follow-up[J]. Front Med(Lausanne), 2015, 39(2): 46-52. [13] Davidson B, Tropé C. Ovarian cancer: diagnostic, biological and prognostic aspects[J]. Womens Health (Lond Engl), 2014, 10(6): 519-33. [14] Castellucci M, Paolo J, Perrone B, et al. Diagnostic accuracy of 18F-FDG PET/CT in characterizing ovarian lesions and staging ovarian cancer: correlation with transvaginal ultrasonography, computed tomography and histology[J]. Nuclear Med Communic, 2018, 28(8): 589-95. [15] Gu P, Pan LL, Wu SQ, et al. CA 125, PET alone, PET-CT, CT and MRI in diagnosing recurrent ovarian carcinoma: a systematic review and meta-analysis[J]. European J Radiol, 2009, 71(1): 164-74. doi: 10.1016/j.ejrad.2008.02.019 [16] Yuan Y, Xiao FT, Gu ZX, et al. Computer tomography, magnetic resonance imaging, and positron emission tomography or positron emission tomography/computer tomography for detection of metastatic lymph nodes in patients with ovarian cancer: a meta-analysis[J]. Europ J Radiol, 2012, 81(5): 1002-6. doi: 10.1016/j.ejrad.2011.01.112 [17] Tanizaki Y, Kobayashi A, Shiro M, et al. Diagnostic value of preoperative SUVmax on FDG-PET/ CT for the detection of ovarian cancer[J]. Int J Gynecol Cancer, 2014, 24(3): 454-60. doi: 10.1097/IGC.0000000000000074 [18] Vargas HA, Burger IA, Goldman DA, et al. Volume-based quantitative FDG PET/CT metrics and their association with optimal debulking and progression-free survival in patients with recurrent ovarian cancer undergoing secondary cytoreductive surgery[J]. Eur Radiol, 2015, 25(11): 3348-53. doi: 10.1007/s00330-015-3729-9 [19] Yamamoto M, Tsujikawa T, Fujita Y, et al. Metabolic tumor burden predicts prognosis of ovarian cancer patients who receive platinum-based adjuvant chemotherapy[J]. Cancer Sci, 2016, 107(4): 478-85. doi: 10.1111/cas.12890 [20] Bono Y, Mizumoto Y, Nakamura M, et al. FDG-PET-positive ovarian thecoma with GLUT5 expression: five cases[J]. J Obstet Gynaecol Res, 2017, 43(3): 599-603. doi: 10.1111/jog.13243 [21] Hynninen J, Auranen A, Olli Carpén, et al. FDG PET/CT in staging of advanced epithelial ovarian cancer: frequency of supradiaphragmatic lymph node metastasis challenges the traditional pattern of disease spread[J]. Gynecol Oncol, 2012, 126(1): 64-8. doi: 10.1016/j.ygyno.2012.04.023 [22] Lv YL, Yuan DM, Wang K, et al. Diagnostic performance of integrated positron emission tomography/computed tomography for mediastinal lymph node staging in non-small cell lung cancer: a bivariate systematic review and meta-analysis[J]. Ajnr Am J Neuroradiol, 2012, 81(5): 1002-6. [23] 盛修贵, 张小玲, 付 政, 等. 正电子发射体层显像-CT检查联合CA125连续检测诊断早期无症状的复发性卵巢上皮性癌的价值[J]. 中华妇产科杂志, 2007, 42(7): 460-3. doi: 10.3760/j.issn:0529-567x.2007.07.008 [24] Zeng J, Yin J, Song X, et al. Reduction of CA125 levels during neoadjuvant chemotherapy can predict cytoreduction to no visible residual disease in patients with advanced epithelial ovarian cancer, primary carcinoma of fallopian tube and peritoneal carcinoma[J]. J Cancer, 2016, 7(15): 2327-32. doi: 10.7150/jca.16761 [25] Montagnana M, Lippi G, Danese E, et al. Usefulness of serum HE4 in endometriotic cysts[J]. British J Cancer, 2009, 101(3): 548-59. doi: 10.1038/sj.bjc.6605119 [26] Azahara PM, José MC, Madel PT, et al. Value of [18F]FDG-PET/CT and CA125, serum levels and kinetic parameters, in early detection of ovarian cancer recurrence: influence of histological subtypes and tumor stages[J]. Medicine, 2018, 97(17): e0098-107. doi: 10.1097/MD.0000000000010098 [27] Crawford SM, Peace J. Does the nadir CA125 concentration predict a long term outcome after chemotherapy for carcinoma of the ovary[J]. Ann Oncol, 2005, 16(1): 47-50. doi: 10.1093/annonc/mdi012 [28] 张 艳, 张菊新. 复发性卵巢癌诊疗进展[J]. 中华实用诊断与治疗杂志, 2013, 27(10): 942-3. [29] Lu KH. Selection of potential markers for epithelial ovarian cancer with gene expression arrays and recursive descent partition analysis[J]. Clin Cancer Res, 2004, 21(10): 3291-300. [30] Galgano MT, Hampton GM, Frierson HF. Comprehensive analysis of HE4 expression in normal and malignant human tissues[J]. Modern Pathol, 2006, 19(11): 327-38. [31] Moore RG, Mcmeekin DS, Brown AK, et al. A novel multiple marker bioassay utilizing HE4 and CA125 for the prediction of ovarian cancer in patients with a pelvic mass[J]. Gynecologic Oncology, 2009, 112(1): 40-6. doi: 10.1016/j.ygyno.2008.08.031 [32] 卢仁泉, 郭 林, 沈烨红. HE4 在卵巢癌诊治中的临床应用评价[J]. 中国癌症杂志, 2010, 20(9): 680-5. doi: 10.3969/j.issn.1007-3639.2010.09.008 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 986
- HTML全文浏览量: 342
- PDF下载量: 10
- 被引次数: 0