



Interim efficacy of ultrasound-guided percutaneous microwave ablation for ≤5 cm breast cancer
-
摘要:
目的 探讨超声引导下经皮微波消融≤5 cm乳腺癌的中期疗效。 方法 回顾性分析2014年1月~2020年12月在我院接受经皮微波消融≤5 cm的42例乳腺浸润性导管癌女性患者。主要终点为肿瘤进展,次要终点包括总体生存率、术后并发症和美容满意度。 结果 42例患者68个癌灶共接受48次消融治疗,完全消融率100%。肿瘤直径2.5±1.2(0.4~5.0)cm。术后随访时间5.0~ 70.5月,中位随访时间29.2月。所有患者术后经超声造影评估均完全消融,1例术后42月发生局部肿瘤进展,1例术后11月发生同侧乳房转移和腋窝淋巴结转移,1例术后29月发生脑转移。消融术后无严重并发症,美容满意度达到100%。 结论 超声引导下经皮微波消融治疗≤5 cm乳腺癌是安全的,尤其为老年女性和患严重合并症的患者提供了微创且可耐受的局部治疗选择。 Abstract:Objective To explore the interim efficacy of ultrasound-guided percutaneous microwave ablation for ≤5 cm breast cancer. Methods Forty-two women with invasive ductal carcinoma of the breast ≤5 cm treated by microwave ablation from January, 2014 to January, 2020 were retrospectively analyzed. The primary end point was tumor progression in the intention-to-treat population. Secondary end points included survival, cosmetic results, and complications. Results The patients received 48 ablation for 68 tumors in evaluated, The complete ablation rate was 100%. The tumor diameter was 2.5±1.2 (0.4-5.0) cm. Median follow-up was 29.2 months (range 5.0-70.5 months). All patients achieved technique effectiveness by contrast-enhanced ultrasound. One local tumor progression, one ipsilateral breast recurrence and one Brain metastases occurred at 42, 11 and 29 months after microwave ablation, respectively. There were no serious complications after ablation, and the patient's aesthetic satisfaction reached 100%. Conclusion Ultrasound-guided percutaneous microwave ablation for ≤ 5 cm breast cancer is safe. It offers a minimally invasive and tolerable local treatment option, especially for older women and patients with severe comorbiditions. -
Key words:
- breast cancer /
- microwaves /
- ablation techniques
-

图 1 64岁女性右乳浸润导管腺癌
A: MWA术前超声显示肿瘤; B: MWA术前超声造影显示肿瘤3.8 cm×2.4 cm; C: MWA术前增强核磁显示肿瘤(白色箭头); D: MWA术后1年显示消融区3.3 cm×1.9 cm; E: MWA术后2 d增强核磁显示肿瘤消融区(白色箭头)肿瘤残骸(黄色箭头); F: MWA术后12月增强核磁显示消融区(白色箭头)肿瘤残骸(黄色箭头)
Figure 1. A 64-year old woman with invasive ductal carcinoma of the right breast.

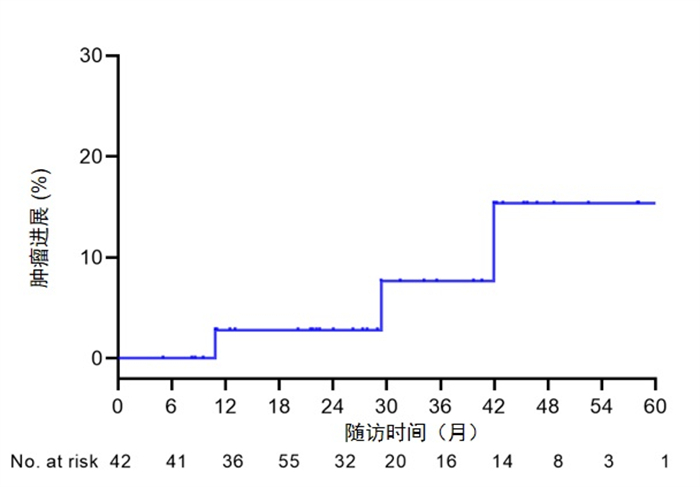
图 2 肿瘤进展的KM曲线
1年、3年和5年的肿瘤进展率2.8%、7.6%和15.4%.
Figure 2. Kaplan-Meier curve of tumor progression Tumor progression rate The 1, 3, 5-year 2.8%, 7.6%, 15.4%.
表 1 患者的一般资料
Table 1. General characteristics for patients in the study group[n(%)]
一般资料 数值 年龄(岁,Mean±SD) 63.7±14.4 查尔森合并指数 3.0(2.0~5.0) 直径(cm,Mean±SD) 2.5±1.2 肿瘤数量 单个 32 (76.2) 多个 10(23.8) 肿瘤位置 左乳 23 (33.8) 右乳 45 (66.2) 肿瘤临近位置 安全 49(72.0) 皮肤 4 (5.9) 乳头 4 (5.9) 胸壁 11(16.2) 消融原因 拒绝手术切除 20(47.6) 失去手术切除机会 22 (52.4) 初发肿瘤 是 33 (78.6) 否 9(21.4) 分子亚型 管腔上皮A型 16(38.1) 管腔上皮B型 管腔上皮B1型 4 (9.5) 管腔上皮B2型 9(21.4) HER2过表达型 6(14.3) 三阴性 2(4.8) 未做分型 5 (11.9)  下载: 导出CSV
下载: 导出CSV
表 2 消融参数
Table 2. Ablation parameters
特征 数值 消融次数[n(%)] 1次 36 (85.7) 2次 6 (14.3) 穿刺次数* 2.0(1.0, 4.0) 消融时间(min)* 12.6(8.4, 19.9) 消融能量(W, Mean±SD) 28.6±6.7 消融淋巴结数量# 0.8 (0.0~7.0) 术后住院时间(d, Mean±SD) 3.0±1.8 住院费用(元, Mean±SD) 24693.8±8222.9 *以中位数(四分位数间距)表示;#以均数(范围)表示.
下载: 导出CSV
表 3 辅助治疗
Table 3. Adjuvant treatment[n(%)]
指标 n (%) 辅助性全身疗法 20 (47.6) 内分泌治疗 7(16.7) 化疗 8 (19.0) 内分泌治疗+化疗 5(11.9) 辅助性放疗 5(11.9) 淋巴结放疗 2 (4.8) 乳腺+淋巴结放疗 3 (7.1)
下载: 导出CSV
表 4 术后结果
Table 4. Postoperative outcomes
结果 n (%) 严重并发症 0(0) 轻微并发症 感染 0(0) 皮肤烫伤 1 (2.4) 美容满意度 非常满意 40 (95.2) 较满意 2 (4.8) 一般 0 (0) 不满意 0 (0) 局部复发 1 (2.4) 同侧乳腺复发 1 (2.4) 前哨淋巴结转移 0 (0) 腋窝淋巴结转移 1 (2.4) 乳腺外转移 1 (2.4) 乳腺癌死亡 0 (0.0) 全因死亡 2 (4.8)
下载: 导出CSV
-
[1] Siegel RL, Miller KD, Fuchs HE, et al. Cancer statistics, 2021[J]. CA Cancer J Clin, 2021, 71(1): 7-33. doi: 10.3322/caac.21654 [2] Fleming MM, Holbrook AI, Newell MS. Update on image-guided percutaneous ablation of breast cancer[J]. AJR Am J Roentgenol, 2017, 208(2): 267-74. doi: 10.2214/AJR.16.17129 [3] Brem RF. Radiofrequency ablation of breast cancer: a step forward [J]. Radiology, 2018, 289(2): 325-6. doi: 10.1148/radiol.2018181784 [4] Lanza E, Palussiere J, Buy X, et al. Percutaneous image-guided cryoablation of breast cancer: a systematic review[J]. J Vasc Interv Radiol, 2015, 26(11): 1652-7. e1. doi: 10.1016/j.jvir.2015.07.020 [5] Peek MCL, Ahmed M, Napoli A, et al. Systematic review of highintensity focused ultrasound ablation in the treatment of breast cancer[J]. Br J Surg, 2015, 102(8): 873-82. doi: 10.1002/bjs.9793 [6] Zhou WB, Jiang YN, Chen L, et al. Image and pathological changes after microwave ablation of breast cancer: a pilot study[J]. Eur J Radiol, 2014, 83(10): 1771-7. doi: 10.1016/j.ejrad.2014.06.015 [7] Zhou WB, Zha XM, Liu XA, et al. US-guided percutaneous microwave coagulation of small breast cancers: a clinical study[J]. Radiology, 2012, 263(2): 364-73. doi: 10.1148/radiol.12111901 [8] Simon CJ, Dupuy DE, Mayo-Smith WW. Microwave ablation: principles and applications[J]. Radiographics, 2005, 25(Suppl 1): S69-S83. [9] EASL clinical practice guidelines: management of hepatocellular carcinoma[J]. J Hepatol, 2018, 69(1): 182-236. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGXH202103001.htm [10] Nault JC, Sutter O, Nahon P, et al. Percutaneous treatment of hepatocellular carcinoma: state of the art and innovations[J]. J Hepatol, 2018, 68(4): 783-97. doi: 10.1016/j.jhep.2017.10.004 [11] Wang Z, Liu M, Zhang DZ, et al. Microwave ablation versus laparoscopic resection as first-line therapy for solitary 3-5-cm HCC [J]. Hepatology, 2022. DOI: 10.1002/hep.32323. [12] Yu J, Zhang X, Liu H, et al. Percutaneous microwave ablation versus laparoscopic partial nephrectomy for cT1a renal cell carcinoma: a propensity-matched cohort study of 1955 patients[J]. Radiology, 2020, 294(3): 698-706. doi: 10.1148/radiol.2020190919 [13] Gardner RA, Vargas HI, Block JB, et al. Focused microwave phased array thermotherapy for primary breast cancer[J]. Ann Surg Oncol, 2002, 9(4): 326-32. doi: 10.1007/BF02573866 [14] Xia LY, Hu QL, Xu WY. Efficacy and safety of radiofrequency ablation for breast cancer smaller than 2 cm: a systematic review and Meta-analysis[J]. Front Oncol, 2021, 11: 651646. doi: 10.3389/fonc.2021.651646 [15] 李永杰, 冯庆亮, 孙凤芝, 等. 超声引导经皮微波热消融和手术切除治疗老年乳腺癌的对照研究[J]. 中国超声医学杂志, 2011, 27(7): 608-11. doi: 10.3969/j.issn.1002-0101.2011.07.011 [16] Palussière J, Henriques C, Mauriac L, et al. Radiofrequency ablation as a substitute for surgery in elderly patients with nonresected breast cancer: pilot study with long-term outcomes[J]. Radiology, 2012, 264(2): 597-605. doi: 10.1148/radiol.12111303 [17] Cazzato RL, de Lara CT, Buy X, et al. Single-centre experience with percutaneous cryoablation of breast cancer in 23 consecutive non-surgical patients[J]. Cardiovasc Intervent Radiol, 2015, 38(5): 1237-43. doi: 10.1007/s00270-015-1181-5 [18] Mauri G, Sconfienza LM, Pescatori LC, et al. Technical success, technique efficacy and complications of minimally-invasive imaging-guided percutaneous ablation procedures of breast cancer: a systematic review and meta-analysis[J]. Eur Radiol, 2017, 27(8): 3199-210. doi: 10.1007/s00330-016-4668-9 [19] Ashikari AY, Kelemen PR, Tastan B, et al. Nipple sparing mastectomy techniques: a literature review and an inframammary technique[J]. Gland Surg, 2018, 7(3): 273-87. doi: 10.21037/gs.2017.09.02 [20] Ito T, Oura S, Nagamine S, et al. Radiofrequency ablation of breast cancer: a retrospective study[J]. Clin Breast Cancer, 2018, 18(4): e495-500. doi: 10.1016/j.clbc.2017.09.007 [21] Liu SS, Cai WJ, Luo YC, et al. CEUS versus MRI in evaluation of the effect of microwave ablation of breast cancer[J]. Ultrasound Med Biol, 2022, 48(4): 617-25. doi: 10.1016/j.ultrasmedbio.2021.11.012 [22] Veronesi U, Paganelli G, Viale G, et al. A randomized comparison of sentinel-node biopsy with routine axillary dissection in breast cancer[J]. N Engl J Med, 2003, 349(6): 546-53. doi: 10.1056/NEJMoa012782 [23] Lyman GH, Giuliano AE, Somerfield MR, et al. American Society of Clinical Oncology guideline recommendations for sentinel lymph node biopsy in early-stage breast cancer[J]. J Clin Oncol, 2005, 23(30): 7703-20. doi: 10.1200/JCO.2005.08.001 [24] Vargas HI, Dooley WC, Gardner RA, et al. Success of sentinel lymph node mapping after breast cancer ablation with focused microwave phased array thermotherapy[J]. Am J Surg, 2003, 186 (4): 330-2. doi: 10.1016/S0002-9610(03)00267-8 -

 点击查看大图
点击查看大图

计量
- 文章访问数: 374
- HTML全文浏览量: 203
- PDF下载量: 34
- 被引次数: 0