



Effect of alprostadil dry emulsion combined with benazepril on the protein level of patients with diabetic nephropathy and its adverse reactions
-
摘要:
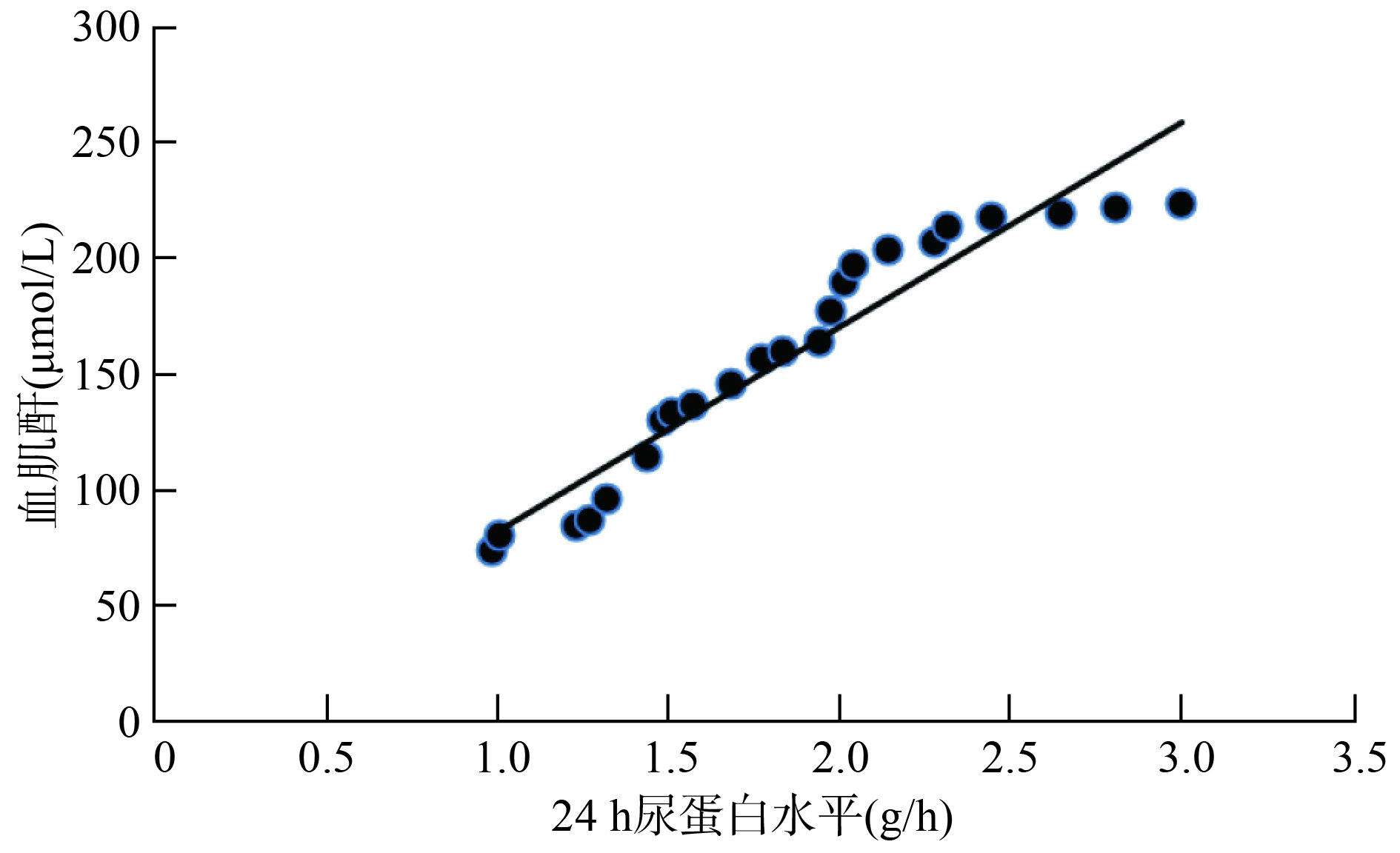
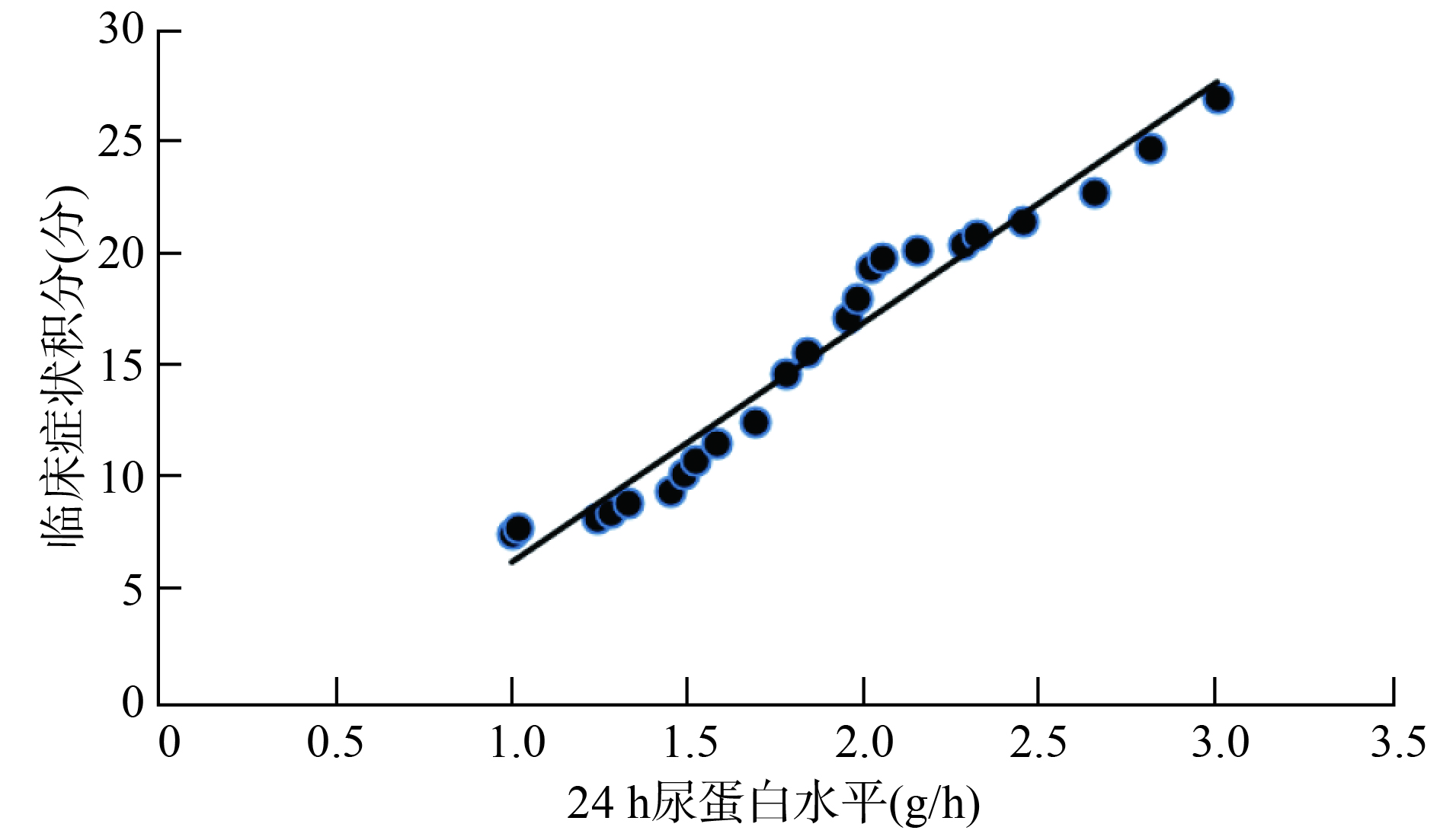
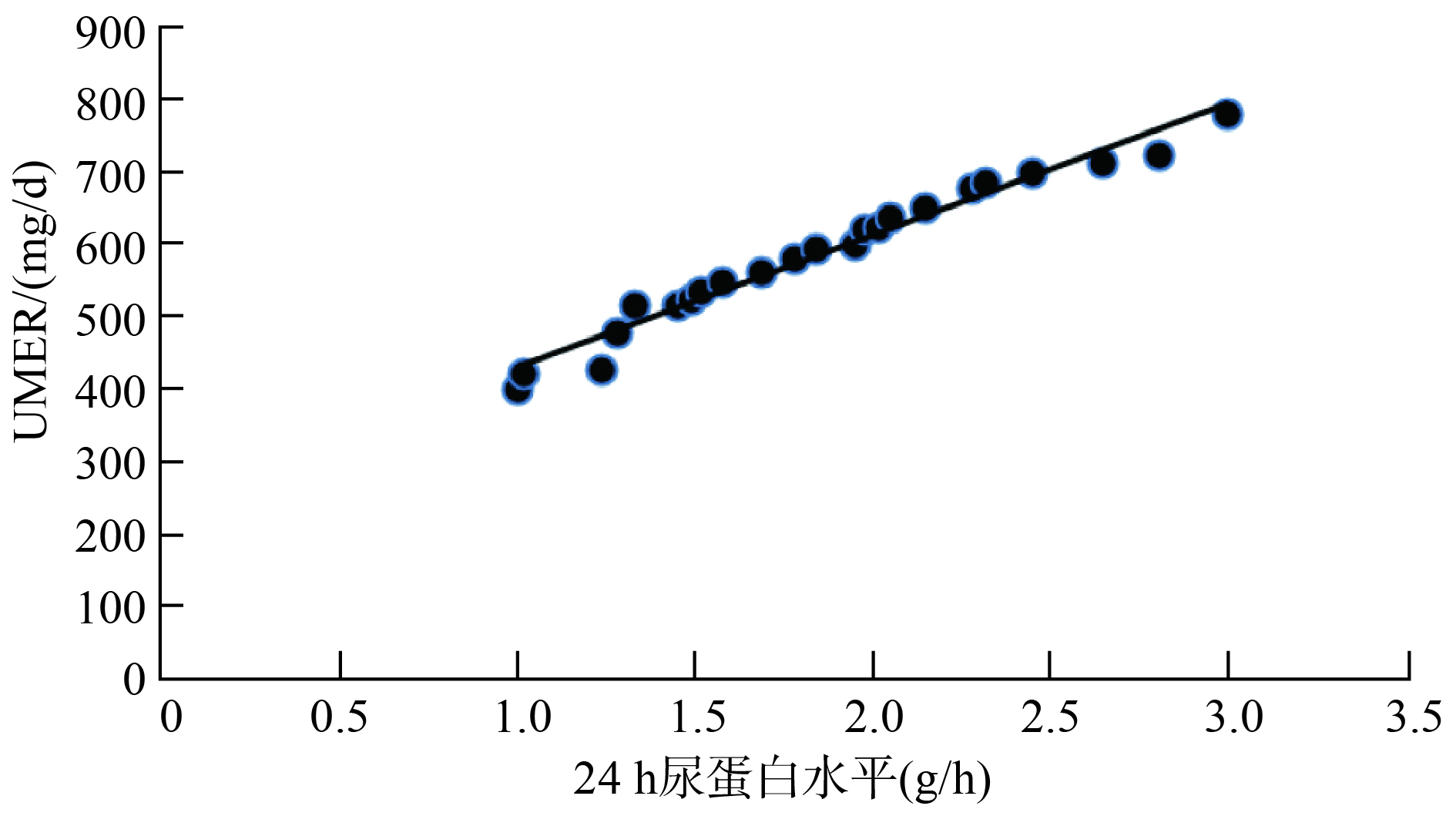
目的 探讨前列地尔干乳剂联合贝那普利对糖尿病肾病患者尿蛋白水平的影响及其不良反应。 方法 将66例糖尿病肾病患者随机分为联合组和对照组(每组33例)。对照组常规行降糖、降压、抗凝和贝那普利口服治疗,联合组在对照组的治疗基础上采用前列地尔前列地尔干乳剂治疗。比较两组疗效,治疗前、治疗2周及4周的24 h尿蛋白水平、24 h尿微白蛋白排泄率(UMER)、血肌酐水平、临床症状积分及治疗期间不良反应发生率,分析24 h尿蛋白水平与UMER、血肌酐水平及临床症状积分的关系。 结果 与对照组相比,联合组治疗显效比例、总治疗有效率提高,治疗2周及4周的24 h尿蛋白水平、UMER、血肌酐水平及临床症状积分则均降低(P<0.05)。与治疗前相比,联合组治疗2周及4周的24 h尿蛋白水平、UMER、血肌酐水平、临床症状积分降低,对照组治疗4周的24 h尿蛋白水平、UMER、血肌酐水平及临床症状积分降低(P<0.05)。两组治疗期间头痛、干咳、恶心、肝肾功能损伤等不良反应发生率差异无统计学意义(P>0.05)。Pearson相关分析显示,接受前列地尔联合贝那普利治疗的糖尿病肾病患者,其24 h尿蛋白水平与UMER、血肌酐水平、临床症状积分呈正相关(r=0.896,0.842,0.763,P<0.05)。 结论 糖尿病肾病患者尿蛋白水平与其肾功能损伤及临床症状均相关,前列地尔联合贝那普利治疗疗效和安全性良好,值得临床推广应用。 Abstract:Objective To explore the effect of alprostadil dry emulsion combined with benazepril on the protein level of patients with diabetic nephropathy and its adverse reactions. Methods 66 patients with diabetic nephropathy were randomly divided into the combination group (n=33) and control group (n=33). Control group received routine hypoglycemic agents, antihypertensive treatment, anticoagulation, and Benazepril by oral administration, while combination group was treated with Alprostadil dry emulsion on the base of the treatment routine of control group, and patients were treated for more than one treatment course. Curative effect, 24 h urine protein level, 24 h urinary microalbumin excretive rate (UMER), serum creatinine level, clinical symptom score and incidence rate of adverse reactions during the treatment of two groups were compared, and the relationship between 24 h urine protein levels with the UMER, serum creatinine level and clinical symptom integral score were analyzed. Results Compared with control group, the proportion of marked therapeutic effect and total curative effect rate of combination group were significantly improved, and 24 h urine protein level, UMER, serum creatinine level, clinical symptom score of combination group before treatment and 2 and 4 weeks after treatment were significantly lower (P<0.05). Compared with those before treatment, 24 h urine protein level, UMER, serum creatinine level, clinical symptom score of combination group 2 and 4 weeks after treatment had significantly decreased, and 24 h urine protein level, UMER, serum creatinine level, clinical symptom score of control group 4 weeks after treatment had also declined (P<0.05). During the treatment phase, no significant differences were found in the incidence rate of adverse reactions, including headache, dry cough, nausea, liver and kidney function damage, between two groups (P>0.05). Pearson correlation analysis results showed that 24 h urine protein level of patients with diabetic nephropathy treated with alprostadil combined with benazepril was positively correlated with UMER, serum creatinine level and clinical symptom integral score (r=0.896, 0.842, 0.896,P<0.05). Conclusion Urine protein level of patients with diabetic nephropathy is associated with renal function injury and clinical symptoms. Alprostadil dry emulsion combined with benazepril has good efficacy and is safe, therefore worthy of clinical popularization and application. -
Key words:
- alprostadil dry emulsion /
- benazepril /
- diabetic nephropathy /
- urine protein /
- adverse reactions
-
表 1 2组临床资料比较(n=33)
组别 性别比(男/女) 年龄(岁,Mean±SD) 病程(年,Mean±SD) 高血压[n(%)] 高脂血症[n(%)] 联合组 18/15 61.89±8.62 4.26±2.08 8(24.24) 13(39.39) 对照组 17/16 62.05±8.97 4.31±2.05 9(27.27) 11(33.33) 统计量 χ2=0.061 t=0.074 t=0.098 χ2=0.079 χ2=0.262 P >0.05 >0.05 >0.05 >0.05 >0.05  下载: 导出CSV
下载: 导出CSV
表 2 2组疗效比较[n=33,n(%)]
组别 显效 有效 无效 总有效率 联合组 18(54.55) 13(39.39) 2(6.06) 31(93.94) 对照组 10(3.03) 15(45.45) 8(24.24) 25(75.76) χ2 3.970 0.248 4.243 4.243 P <0.05 >0.05 <0.05 <0.05
下载: 导出CSV
表 3 联合组和对照组治疗前后24 h尿蛋白水平、UMER、血肌酐水平比较(n=33, Mean±SD)
因子 组别 治疗前 治疗2周 治疗4周 24 h尿蛋白水平(g/d) 联合组 2.52±0.55 1.74±0.35*# 1.29±0.22*# 对照组 2.54±0.53 2.38±0.48 1.85±0.38* UMER(mg/d) 联合组 739.96±48.92 655.53±43.18*# 422.28±32.85*# 对照组 741.18±50.55 734.69±46.48 598.62±36.99* 血肌酐(μmol/L) 联合组 186.77±22.48 145.78±12.25*# 85.56±11.18*# 对照组 185.12±20.37 176.36±18.77 102.42±13.66* *P<0.05vs同组治疗前; #P<0.05vs对照组; UMER: 尿蛋白排泄率.
下载: 导出CSV
表 4 联合组和对照组治疗前后临床症状积分比较(分,n=33,Mean±SD)
组别 治疗前 治疗2周 治疗4周 联合组 22.68±4.68 13.44±3.25*# 10.24±3.11*# 对照组 22.39±4.53 20.25±4.18 14.75±3.42* t 0.256 7.389 5.605 P >0.05 <0.05 <0.05 *P<0.05vs同组治疗前; #P<0.05vs对照组.
下载: 导出CSV
表 5 联合组和对照组不良反应发生率比较[n=33,n(%)]
组别 头痛 干咳 恶心 肝肾功能损伤 总有效率 联合组 0(0.00) 2(6.06) 2(6.06) 0(0.00) 4(12.12) 对照组 1(3.03) 2(6.06) 1(3.03) 0(0.00) 5(15.15) χ2 0.000 0.266 0.000 0.000 0.000 P >0.05 >0.05 >0.05 >0.05 >0.05
下载: 导出CSV
-
[1] Oe Y, Hayashi S, Fushima T, et al. Coagulation factor Xa and Protease-Activated receptor 2 as novel therapeutic targets for diabetic nephropathy[J]. Arterioscler Thromb Vasc Biol, 2016, 36(8): 1525-33. [2] 马金玲. 贝那普利联合金水宝对糖尿病肾病蛋白尿患者的临床治疗效果观察[J]. 继续医学教育, 2018, 32(5): 155-7. [3] 钟裕元, 李会珍, 张秋彬. 补肾益气汤联合西药治疗Ⅳ期糖尿病肾病(气阴两虚)随机平行对照研究[J]. 实用中医内科杂志, 2018, 32(4): 28-31. [4] 邱丹丹, 蒋 松, 潘 瑜, 等. 血磷水平与糖尿病肾病患者肾脏损伤及远期预后的关系[J]. 肾脏病与透析肾移植杂志, 2016, 25(3): 208-13. [5] 贺建杰, 黄喜桃. 贝那普利与前列地尔联合治疗糖尿病肾病蛋白尿的临床效果[J]. 临床医学研究与实践, 2018, 3(10): 34-5. [6] 化宝军. 前列地尔联合贝那普利治疗糖尿病肾病蛋白尿的临床效果分析[J]. 中国实用医药, 2015, 10(16): 139-40. [7] Jin H, Piao SG, Jin JZ, et al. Synergistic effects of leflunomide and benazepril in streptozotocin-induced diabetic nephropathy[J]. Nephron Exp Nephrol, 2014, 126(3): 148-56. [8] 李英昭, 张秋萍. 前列地尔治疗老年早期糖尿病肾病的临床研究[J]. 实用药物与临床, 2013, 16(4): 290-2. [9] 郑筱萸. 中药新药临床研究指导原则(试行)[S]. 北京: 中国医药科技出版社, 2002. [10] 褚家礼, 刘丽娟. 前列地尔联合贝那普利治疗糖尿病肾病蛋白尿的临床效果分析[J]. 糖尿病新世界, 2015, 35(6): 25-25, 27. [11] 李春桂, 苗桂珍, 朱学敏. 益气养阴清热活血法治疗早期糖尿病肾病33例临床观察[J]. 河北中医, 2009, 31(8): 1133-5. [12] 安 玉. 糖尿病肾病病理改变与预后的关系[J]. 肾脏病与透析肾移植杂志, 2013, 22(4): 368-72. [13] 柴东林, 庞 涛. 瑞舒伐他汀联合贝那普利对老年糖尿病肾病患者血清肌肝、尿素氨水平变化的影响[J]. 中国药物与临床, 2018, 18(2): 244-6. [14] Peng T, Chang X, Wang J, et al. Protective effects of tacrolimus on podocytes in early diabetic nephropathy in rats[J]. Mol Med Rep, 2017, 15(5): 3172-8. [15] Dong XG, An ZM, Guo Y, et al. Effect of triptolide on expression of oxidative carbonyl protein in renal cortex of rats with diabetic nephropathy[J]. J Huazhong Univ Sci Technolog Med Sci, 2017, 37(1): 25-9. [16] 王俊坦. 腹膜转运特性与糖尿病肾病腹膜透析患者预后的关系[J]. 现代仪器与医疗, 2016, 22(4): 114-5, 120. [17] 窦华林. 贝那普利和阿托伐他汀联用对2型糖尿病并发肾病的治疗效果研究[J]. 北方药学, 2018, 15(4): 36-7. [18] Luo C, Li T, Zhang C, et al. Therapeutic effect of alprostadil in diabetic nephropathy: possible roles of angiopoietin-2 and IL-18[J]. Cell Physiol Biochem, 2014, 34(3): 916-28. [19] 刘玉玲. 前列地尔联合贝那普利治疗糖尿病肾病蛋白尿[J]. 临床医学, 2016, 36(7): 36-8. [20] 汤 靓. 前列地尔联合贝那普利治疗糖尿病肾病蛋白尿的疗效[J]. 中国医药指南, 2018, 16(11): 110-4. [21] 李景萍. 贝那普利联合缬沙坦治疗糖尿病肾病的效果观察[J]. 数理医药学杂志, 2018, 31(4): 563-4. [22] 潘美时. 前列地尔联合贝那普利治疗糖尿病肾病蛋白尿30例[J]. 中国药业, 2015, 24(15): 117-8. [23] Generali JA, Cada DJ. Benazepril: nephropathy (non-diabetic) [J]. Hosp Pharm, 2016, 51(4): 293-5. [24] 林 芳. 前列地尔联合贝那普利治疗糖尿病肾病蛋白尿的临床效果分析[J]. 中国医药指南, 2016, 14(2): 87-8. [25] 张国艳, 张 浩, 牛效清. 前列地尔联合贝那普利治疗糖尿病肾病蛋白尿的疗效[J]. 当代医学, 2012, 18(4): 145-6. -

 点击查看大图
点击查看大图
图(3) / 表(5)
计量
- 文章访问数: 2264
- HTML全文浏览量: 832
- PDF下载量: 4
- 被引次数: 0