



Diagnostic value of HRCT, routine and functional MRI in low-grade chondrosarcoma of skull base
-
摘要:
目的探讨高分辨率CT(HRCT)、常规及功能MRI对颅底软骨肉瘤的诊断价值。 方法回顾性分析10例病理证实的颅底低级别(Ⅰ~Ⅱ级)软骨肉瘤患者的HRCT及MRI图像。MRI扫描序列包括常规T1WI、T2WI、弥散加权成像、动态增强磁共振成像(DCE-MRI)及磁共振波谱成像(MRS)。HRCT主要观察病灶骨质破坏及钙化。常规MRI上主要观察病灶形状、大小、位置、累及范围及信号特点。功能MRI上测量病灶的表观弥散系数及DCE-MRI参数:时间信号曲线(TIC)类型、最高强化率及达峰时间,MRS上主要观察胆碱峰(Cho)/肌酸峰(Cr)比值以及有无N-乙酰天门冬氨酸峰(NAA)。 结果HRCT上10例均出现虫蚀样骨质破坏,6例出现钙化,钙化表现为点状、不规则斑片状。MRI上所有肿瘤(10/10)形态不规则,平均大小为3.5 cm×3.0 cm× 4.2 cm。10例中,8例肿瘤主体位于颈静脉孔区,2例病灶主体位于颞骨乳突部。肿瘤累及周围结构主要包括颈静脉孔(n=8)、面神经管鼓室段及乳突段(n=8)、颞骨乳突部(n=7)、中耳(n=5)、舌下神经管(n=4)、咽旁间隙及腮腺深叶(n=4)、颈动脉间隙(n= 3)、桥小脑角区(n=1)。10例病灶T1WI上呈均匀等信号,T2WI上呈明显不均匀高信号,增强后呈不均匀轻中度强化。10例病灶平均表观弥散系数值为(1.96±0.10)×10-3 mm2/s。10例病灶DCE-MRI的TIC均呈持续上升型(Ⅰ型曲线),最高强化率1.20± 0.44,达峰时间均≥210 s。10例病灶MRS上Cho峰/Cr峰比值均小于1,未见明显NAA峰。 结论颅底发生虫蚀样骨质破坏伴不规则形软组织肿块,HRCT内部见钙化,T2WI信号呈明显不均匀高信号,增强后不均匀轻中度强化,功能成像弥散加权成像显示弥散不受限,TIC呈Ⅰ型,MRS上Cho峰/Cr峰比值小于1,无明显NAA峰则提示软骨肉瘤诊断的可能性。 Abstract:ObjectiveTo explore the diagnostic value of high resolution CT (HRCT), routine and functional MRI in low grade chondrosarcoma of skull base. MethodsThe HRCT and MR images of 10 patients with pathologically proved low grade chondrosarcoma of the skull base (grade Ⅰ-Ⅱ) were retrospectively analyzed. The sequences of MRI scan included conventional T1WI, T2WI, DWI, DCE-MRI and MR spectroscopy (MRS). Bone destruction and calcification were mainly observed on HRCT. The shape, size, location, involvement range and signal characteristics of the lesions were analyzed on routine MRI. Apparent diffusion coefficient (ADC) and DCE-MRI parameters including time intensity curve (TIC), maximum ratio of enhancement (ERmax) and time to peak (TTP) were measured on functional MRI. The Cho/Cr peak ratio and the presence or absence of NAA peak were observed on MRS. Results Bone destruction characterized by mouse nibbled was found in all tumors (10/10) on HRCT. 6 cases showed calcification which was punctuate and irregular patchy. All tumors (10/10) were irregular with an average size of 3.5 cm ×3.0 cm ×4.2 cm. Eight of the 10 cases were located in jugular foramen and two in temporal mastoid region. The surrounding structures were mainly involved in jugular foramen (n=8), tympanic and mastoid segments of facial nerve canal (n=8), mastoid portion of temporal bone (n=7), middle ear (n=5), hypoglossal canal (n=4), parapharyngeal space and deep parotid lobe (n=4), carotid artery space (n=3), and cerebellopontine angle area (n=1). Ten lesions showed homogeneous isointensity on T1WI and inhomogeneous hyperintensity on T2WI. And after enhancement, the lesions showed inhomogeneous mild to moderate enhancement. The average ADC value of 10 lesions was (1.96±0.10)×10-3 mm2/s. The TIC of DCE-MRI in 10 cases showed a continuous ascending pattern (type Ⅰ), with ERmax=1.20±0.44 and TTP (≥210 s). The ratio of Cho peak to Cr peak on MRS of 10 lesions was less than 1, and no obvious NAA peak was found. ConclusionSkull base bone destruction characterized by mouse nibbled with irregular soft tissue mass, which showed calcification on HRCT and obviously inhomogeneous high signal on T2WI, inhomogeneous mild to moderate enhancement after enhancement, unlimited dispersion on DWI, type Ⅰ TIC and the value of Cho/Cr on MRS was less than 1, no obvious NAA peak suggested the possibility of diagnosis of chondrosarcoma. -
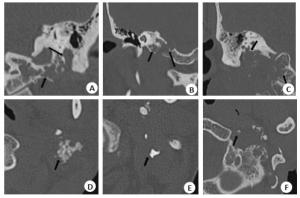
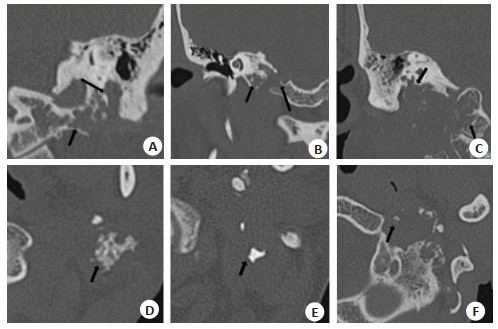
图 1 颅底低级别软骨肉瘤的HRCT表现
不同患者软骨肉瘤的HRCT表现, 颞骨乳突部和岩部、枕骨可见多部位虫蚀样骨质破坏(A~C, 黑箭头); 病灶内部混杂点状, 不规则斑片状钙化灶, 其密度浓淡不一(D~F, 黑箭头)
Figure 1. HRCT findings of low grade chondrosarcoma of skull base
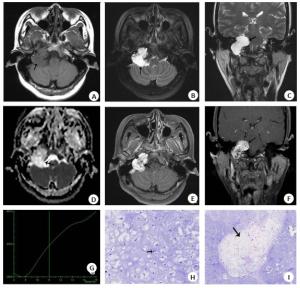
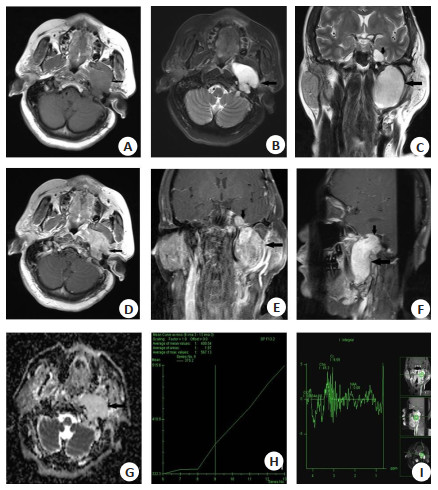
图 2 女,42岁,右侧颅底、颈静脉孔区低级别软骨肉瘤
T1WI上呈等信号(A, 黑箭), T2WI上明显高信号(B~C, 黑箭).ADC图呈高信号, 肿块ADC值为1.98×10-3 mm2/s(D, 黑箭). 增强可见明显不均匀强化(E~F, 黑箭). DCE-MRI TIC呈持续上升型(Ⅰ型),ERmax为1.22, TTP≥210 s(G). HE染色镜下可见成片软骨样细胞, 细胞有异型性(H, 黑箭, HE×400)及部分区域间质疏松(I, 黑箭, HE×40).
Figure 2. Female, 42 years old, with low grade chondrosarcoma of right skull base and jugular foramen area
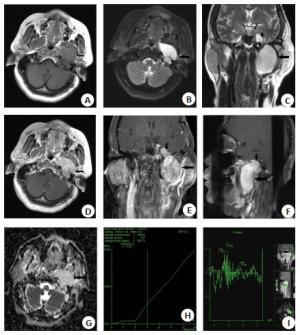
图 3 女,56岁,左侧颅底、颈静脉孔区低级别软骨肉瘤
T1WI上呈等信号(A, 黑箭); T2WI上明显高信号(B~C, 黑箭), 局部累及左侧海绵窦区(C, 黑短箭); 增强可见较不均匀强化(D~F, 黑箭), 局部累及左侧颈静脉孔区(F, 黑短箭); ADC图呈高信号, 肿块ADC值为1.83×10-3 mm2/s(G, 黑箭); DCE-MRI TIC呈持续上升型(Ⅰ型), ERmax为0.96, TTP≥210s(H); MRS上NAA峰不明显, Cho峰/Cr峰比值小于1(I).
Figure 3. Female, 56 years old, with low grade chondrosarcoma of left skull base and jugular foramen area
表 1 10例颅底软骨肉瘤临床资料及MRI表现
Table 1. Clinical data and MR findings of 10 cases of chondrosarcoma of skull base
编号 性别 年龄(岁) 病程 症状 ADC(×10-3 mm2/s) TIC ERmax TTP(s) Cho/Cr NAA 1 女 26 12月 面瘫 1.90 Ⅰ型 1.24 ≥210 < 1 无 2 男 65 4年 面瘫、听力下降、头痛、声嘶、声带麻痹 2.01 Ⅰ型 0.69 ≥210 < 1 无 3 男 40 2月 鼻塞 1.84 Ⅰ型 0.85 ≥210 < 1 无 4 女 42 3年 右听力下降、声嘶、饮水呛咳 1.98 Ⅰ型 1.22 ≥210 < 1 无 5 女 45 10年 左耳鸣、听力下降伴口角歪斜 1.92 Ⅰ型 1.67 ≥210 < 1 无 6 女 60 28年 左面瘫、耳痛 2.0 Ⅰ型 0.91 ≥210 < 1 无 7 女 34 4月 头痛、头晕、伴听力下降 2.2 Ⅰ型 1.02 ≥210 < 1 无 8 女 58 7年 耳鸣、流液、听力下降、声嘶 1.83 Ⅰ型 0.96 ≥210 < 1 无 9 男 51 6月 头痛、头晕 1.98 Ⅰ型 1.50 ≥210 < 1 无 10 男 31 3月 伸舌左偏 1.93 Ⅰ型 2.21 ≥210 < 1 无  下载: 导出CSV
下载: 导出CSV
-
[1] Brackmann DE, Teufert KB. Chondrosarcoma of the skull base: longterm follow-up[J]. Otol Neurotol, 2006, 27(7): 981-91. doi: 10.1097/01.mao.0000233812.48800.b4 [2] 张芳, 段小慧, 温学花, 等. 颅底颌面部黏液型软骨肉瘤CT和MRI表现[J]. 实用放射学杂志, 2014, 30(1): 44-8, 68. doi: 10.3969/j.issn.1002-1671.2014.01.010 [3] 卢红, 王健, 蔡萍, 等. 颅底高分化软骨肉瘤的CT及MRI诊断价值[J]. 中国医学影像学杂志, 2017, 25(7): 501-4. doi: 10.3969/j.issn.1005-5185.2017.07.005 [4] Abdel Razek AAK, Poptani H. MR spectrsocopy of head and neck cancer[J]. Eur J Radiol, 2013, 82(6): 982-9. doi: 10.1016/j.ejrad.2013.01.025 [5] 陶晓峰, 李谊, 徐雪元, 等. 眼眶肿瘤的氢质子磁共振波谱的临床应用研究[J]. 放射学实践, 2008, 23(5): 479-82. doi: 10.3969/j.issn.1000-0313.2008.05.005 [6] Yang B T, Wang Y Z, Dong J Y, et al. MRI study of solitary fibrous tumor in the orbit[J]. AjrAm J Roentgenol, 2012, 199(4): 506-11. doi: 10.2214/AJR.11.8477 [7] Neff B, Sataloff RT, Storey L, et al. Chondrosarcoma of the skull base [J]. Laryngoscope, 2002, 112(1): 134-9. doi: 10.1097/00005537-200201000-00023 [8] Rosenberg A, Nielsen P, Keel SB, et al. Chondrosarcomas of the base of skull[J]. Am J Surg Path, 1999, 23: 1370-8. doi: 10.1097/00000478-199911000-00007 [9] Seidman MD, Nichols RD, Raju UB, et al. Extracranial skull base chondrosarcoma[J]. Ear Nose Throat J, 1989, 68(8): 626-32, 635. http://europepmc.org/abstract/MED/2684602 [10] Raghu M, Moumoulidis I, De R, et al. Chondrosarcomas of the temporal bone: presentation and management[J]. J Laryngol Otol, 2004, 118(7): 551-5. doi: 10.1258/0022215041615272 [11] 王慧芳, 周永杰, 周克阳, 等. 颅底软骨肉瘤CT与MRI表现(附4例报告)[ J]. 实用放射学杂志, 2015(6): 1041-2, 1045. doi: 10.3969/j.issn.1002-1671.2015.06.045 [12] Lustig LR, Sciubba J, Holliday MJ. Chondrosarcomas of the skull base and temporal bone[J]. J Laryngol Otol, 2007, 121(8): 725-35. doi: 10.1017/S0022215107006081 [13] Yeom KW, Lober RM, Mobley BC, et al. Diffusion-weighted MRI: distinction of skull base chordoma from chondrosarcoma[J]. AJNR Am J Neuroradiol, 2013, 34(5): 1056-61. doi: 10.3174/ajnr.A3333 [14] de Carvalho Rangel C, Hygino Cruz LC Jr, Takayassu TC Jr, et al. Diffusion MR imaging in central nervous system[J]. Magn Reson Imaging Clin NAm, 2011, 19(1): 23-53. doi: 10.1016/j.mric.2010.10.006 [15] Abdel Razek A, Mossad A, Ghonim M. Role of diffusion-weighted MR imaging in assessing malignant versus benign skull-base lesions [J]. Radiol Med, 2011, 116(1): 125-32. doi: 10.1007/s11547-010-0588-y [16] White ML, Zhang Y, Robinson RA. Evaluating tumors and tumorlike lesions of the nasal cavity, the paranasal sinuses, and the adjacent skull base with diffusion-weighted MRI[J]. J Comput Assist Tomogr, 2006, 30(3): 490-5. doi: 10.1097/00004728-200605000-00023 [17] Srinivasan A, Dvorak R, Perni K, et al. Differentiation of benign and malignant pathology in the head and neck using 3T apparent diffusion coefficient values: early experience[J]. AJNR Am J Neuroradiol, 2008, 29(1): 40-4. doi: 10.3174/ajnr.A0743 [18] Ginat DT, Mangla R, Yeaney G, et al. Diffusion-weighted imaging for differentiating benign from malignant skull lesions and correlation with cell density[J]. AJR Am J Roentgenol, 2012, 198 (6): W597-601. doi: 10.2214/AJR.11.7424 [19] Müller U, Kubik-Huch RA, Ares C, et al. Is there a role for conventional MRI and MR diffusion-weighted imaging for distinction of skull base chordoma and chondrosarcoma?[J]. Acta Radiol, 2016, 57(2): 225-32. doi: 10.1177/0284185115574156 [20] 郑婉静, 曹代荣, 邢振, 等. 对比分析颅底软骨肉瘤与脊索瘤CT和MRI征象[J]. 中国医学影像技术, 2018, 34(11): 1699-702. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYXX201811036.htm [21] 曾莉, 刘衡, 李亚英, 等. DWI对颅底脊索瘤与软骨肉瘤鉴别诊断的应用价值[J]. 实用放射学杂志, 2017, 33(6): 528-31, 542. doi: 10.3969/j.issn.1002-1671.2017.06.003 [22] Welzel T, Meyerhof E, Uhl M, et al. Diagnostic accuracy of DW MR imaging in the differentiation of chordomas and chondrosarcomas of the skull base: a 3.0-T MRI study of 105 cases[J]. Eur J Radiol, 2018, 105: 119-24. doi: 10.1016/j.ejrad.2018.05.026 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 1168
- HTML全文浏览量: 610
- PDF下载量: 11
- 被引次数: 0