



Radiography features of children patients with severe adenovirus pneumonia in different stages
-
摘要:
目的 探讨儿童重症腺病毒肺炎不同阶段影像学特征与临床表现的相关性。 方法 回顾性分析2016年1月~2017年12月入住我院重症监护室的31例重症腺病毒肺炎病例,将患儿病程分为急性期(起病1月内)、恢复早期(起病1~6月)和恢复后期(起病6月后)3个阶段,分析急性期患儿胸片病变范围与反映肺损伤严重程度的氧和指数的相关性;分析恢复期胸部CT特征与临床表现的相关性。 结果 31例患儿中25例<2岁,6例≥2岁,所有重症腺病毒肺炎患儿急性期均有持续高热、喘息气促症状,白细胞计数多在正常范围或降低,胸片改变早期主要表现双肺内带散在斑片影,随病情进展,肺部渗出快速向中外带发展,呈现肺段及大叶性肺实变,患儿胸片病灶范围越大,其肺损伤程度越重;胸片病灶范围与机械通气时间、ICU住院时间、死亡率呈正相关(P<0.05),但与总住院时间无明显相关性(P>0.05)。死亡4例均发生在急性期,15例患儿在恢复期行胸部CT检查,11例在恢复早期即表现为肺部”马赛克”征伴反复咳喘症状,在恢复后期喘息症状虽减轻,但复查胸部CT无改善,这11例患儿中<2岁10例,≥2岁仅1例,另有1例<2岁患儿恢复期后期CT表现为支气管扩张和单侧透明肺,其余3例患儿恢复期胸部CT基本恢复正常。 结论 儿童重症腺病毒肺炎急性期胸部X片改变可较准确反映病情严重程度与进展情况,与预后相关;而恢复期伴肺部后遗症患儿胸部CT典型“马赛克”征可长期存在,<2岁患者可能较≥2岁患者在恢复期更容易发生肺部后遗症。 Abstract:Objective To explore the imaging characteristics of children with severe adenovirus pneumonia in different stages. Methods Retrospective analysis of 31 cases of severe adenovirus pneumonia in pediatrics intensive care unit from January 2016 to December 2017 was conducted. The course of the disease was divided into 3 stages including acute, early recovery and late recovery stage.We compared the clinical manifestations and imaging features of children in different stages. Results Twenty-five were younger than 2 years old. All the patients had persistent high fever, wheezing and tachypnea in acute stage. The counts of WBC was normal or lower. Chest X-ray early mainly manifested effusion in bilateral lung inner zone, with the disease deteriorated, pulmonary effusion rapidly developmented. The exudation of X-ray in different children was consistent with the severity of lung injury, which was consistent with the condition grew worse in one patient. Four cases died in acute stage. CT was performed in 15 children during the recovery period. Eleven children’s CT showed uneven" mosaic perfusion”in early revcovery stage. Although wheeze alleviated, CT had no improvement in the later recovery stage. Bronchial dilation and hyaline membrane lesions has been showed in 1 cases. Conclusion The size and the density of chest X-ray in acute stage of severe adenovirus pneumonia in children is closely related to the severity and development of the disease. The children younger than 2 years old more likely have the symptoms of continuous cough and wheeze in recovery period. Lung CT showed" mosaic perfusion”of occlusive bronchiolitis may exist for a long time. -
Key words:
- adenovirus /
- severe pneumonia /
- radiology
-

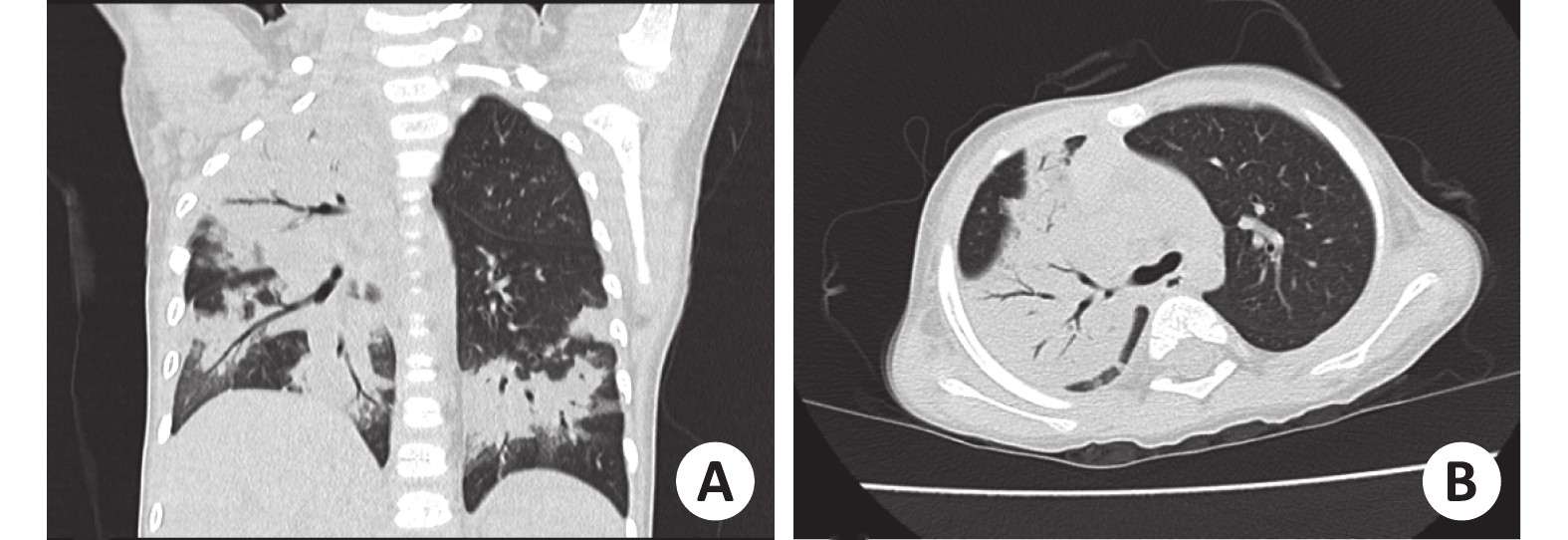
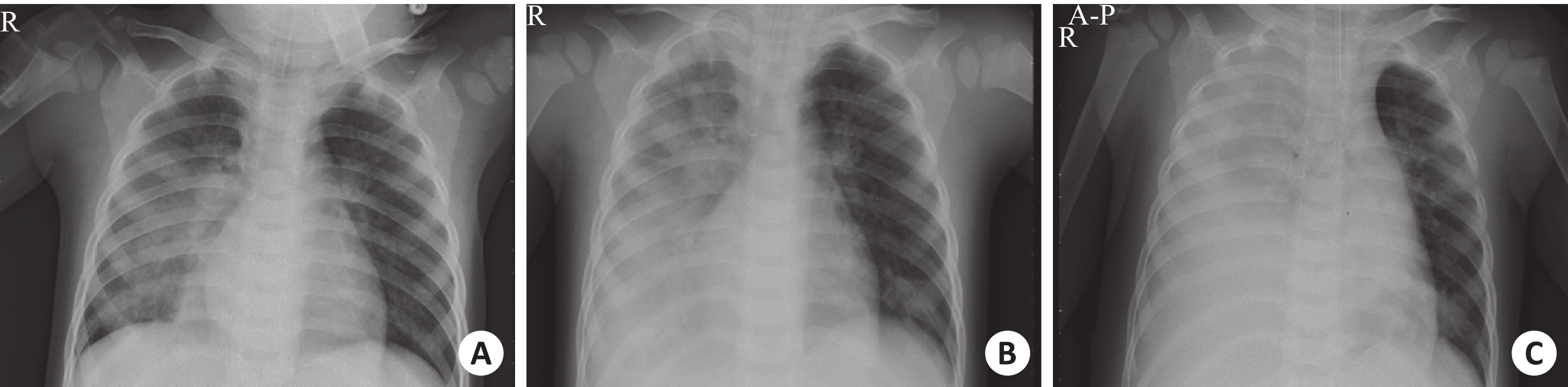
图 1 患儿胸部X片
男,1岁9月,因“发热、咳嗽3 d,气促1 d”收入重症监护室;A:入室后第1天,左肺内带及右肺中内带斑片状模糊影,以右肺中叶下肺野为著;B:入室后第2天,右肺病灶范围较前扩大,伴右侧胸腔积液;C:入室后第4天,右肺病灶进一步加重,近乎白肺改变.
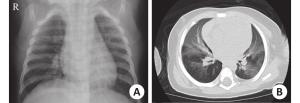
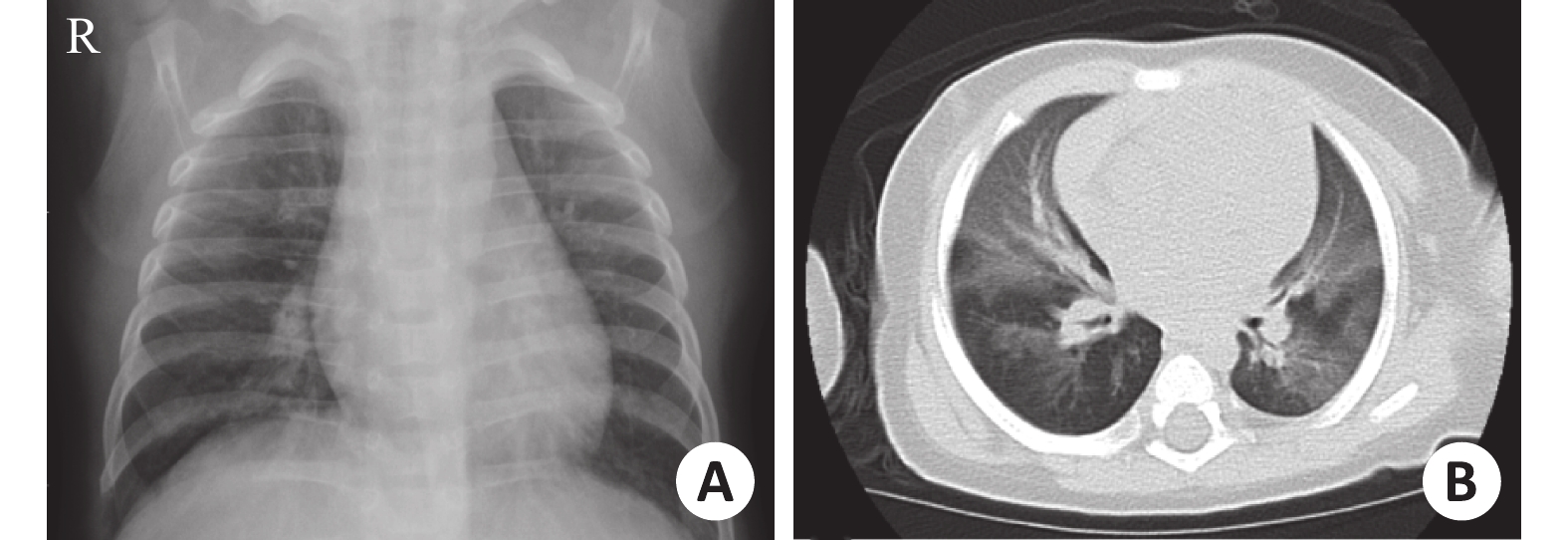
图 3 恢复早期
患儿,男,7月大,因“反复咳喘3月余”复诊,3月前因“重症ADV感染”入住重症监护室,行机械通气治疗;A:X线平片,双肺纹理增多、增粗,考虑支气管炎;B:高分辨CT,双肺透亮度不均匀,可见“马赛克”样改变.

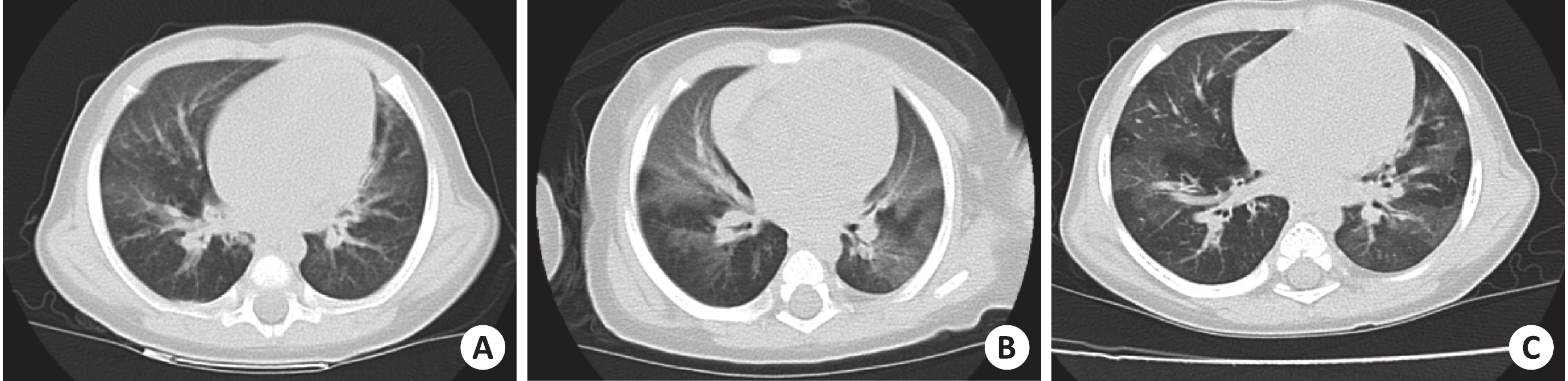
图 4 重症ADV肺炎后复查胸部CT
患儿,男,均可见不均匀充气征,”马赛克”征无明显改善;A:重症ADV肺炎后1月;B;重症ADV肺炎后4月;C:重症ADV肺炎后10月.
表 1 肺部氧合指数与胸片渗出范围分级的相关性
氧合指数 胸片渗出范围分级 合计 1级 2级 3级 轻度(200~300) 6 1 0 7 中度(100~200) 0 9 5 14 重度(<100) 0 0 10 10 合计 6 10 15 31 P=0.001, r=0.728.  下载: 导出CSV
下载: 导出CSV
表 2 存活患儿机械通气时间、ICU住院时间、总住院时间与胸片渗出范围的相关性(Mean±SD)
指标 胸片渗出范围分级 P r 1级(n=6) 2级(n=9) 3级(n=12) 机械通气时间(d) 3.67±2.73 6.56±4.95 18.67±10.60 0.001 0.636 ICU住院时间(d) 7.33±2.42 9.78±5.43 24.75±17.77 0.011 0.523 总住院时间(d) 30±16.38 28±9.87 40.5±24.28 0.302 0.255
下载: 导出CSV
表 3 不同年龄阶段重症腺病毒肺炎患儿预后情况
病情阶段 预后 <2岁 ≥2岁 合计 χ2 P 急性期 28 d死亡率 12%(3/25) 16.7%(1/6) 12.9%(4/31) 0.094 0.759 恢复期 肺部后遗症发生率 50%(11/22) 20%(1/5) 44.4%(12/27) 1.485 0.223
下载: 导出CSV
-
[1] Hong JY, Lee HJ, Piedra PA, et al. Lower respiratory tract infections due to adenovirus in hospitalized Korean children: epidemiology, clinical features, and prognosis[J]. Clin Infect Dis, 2001, 32(10): 1423-9 doi: 10.1086/320146 [2] 贾鑫磊, 钱素云. 儿童重症腺病毒肺炎[J]. 中国小儿急救医学, 2015, 22(12): 814-7 doi: 10.3760/cma.j.issn.1673-4912.2015.12.002 [3] Shen CF, Wang SM, Ho TS, et al. Clinical features of community acquired adenovirus pneumonia during the 2011community outbreak in Southern Taiwan:role of host immune response[J]. BMC Infect Dis, 2017, 17(1): 196-204 doi: 10.1186/s12879-017-2272-5 [4] 李 燕, 何 玲, 陈 欣, 等. 56例儿童重症ADV肺炎的胸部CT影像表现特点[J]. 第三军医大学学报, 2012, 34(6): 558-60 [5] 尹丹萍, 李 理, 孙 刚. 儿童闭塞性细支气管炎的临床及高分辨率CT特点[J]. 中华消化病与影像杂志(电子版), 2017, 7(4): 150-2 doi: 10.3877/cma.j.issn.2095-2015.2017.04.002 [6] 中华医学会儿科学分会呼吸学组, 中华儿科杂志编辑委员会. 儿童社区获得性肺炎管理指南(2013年修订)(上)[J]. 中华儿科杂志, 2013, 51(10): 745-52 doi: 10.3760/cma.j.issn.0578-1310.2013.10.006 [7] Ranieri VM, Rubenfeld GD, Thompson B, et al. Acute respiratory distress syndrome the Berlin definition[J]. JAMA, 2012, 307(23): 2526-33 [8] 曹玉书, 张志良, 王 施, 等. 成人重症ADV肺炎胸部CT动态变化[J]. 实用放射学杂志, 2015, 31(9): 1447-9 doi: 10.3969/j.issn.1002-1671.2015.09.010 [9] Kern S, Uhl M, Berner R, et al. Respiratory syncytial virus infection of the lower, respiratory tract: radiological findings in 108 children[J]. Eur Radiol, 2001, 11(12): 2581-4 doi: 10.1007/s003300100887 [10] Kim YN, Cho HJ, Cho YK, et al. Clinical significance of pleural effusion in the new influenza A (H1N1) viral pneumonia in children and adolescent[J]. Pediatr Pulmonol, 2012, 47(5): 505-9 doi: 10.1002/ppul.21588 [11] 胡亚美, 江载芳, 申昆玲, 等. 诸福棠实用儿科学[M]8版. 北京: 人民卫生出版社, 2015: 1268-72. [12] Lai CY, Lee CJ, Lu CY, et al. Adenovirus serotype 3 and 7 infection with acute respiratory failure in children in Taiwan, 2010-2011[J]. PLoS One, 2013, 8(1): 53614-22 doi: 10.1371/journal.pone.0053614 [13] Tsou TP, Tan BF, Chang HY, et al. Community outbreak of adenovirus, Taiwan, 2011[J]. Emerg Infect Dis, 2012, 18(11): 1825-32 doi: 10.3201/eid1811.120629 [14] Frush DP. CT dose and risk estimates in children[J]. Pediatr Radiol, 2011, 41(9): 483-7 [15] Westra SJ. The communication of the radiation risk from CT in relation to its clinical benefit in the era of personalized medicine:part 1:the radiation risk from CT[J]. Pediatr Radiol, 2014, 44(10): 515-8 [16] Pediatric Acute Lung Injury Consensus Conference Group. Pediatric acute respiratory distress syndrome:consensus recommendations from the Pediatric Acute Lung Injury Consensus Conference[J]. Pediatr Crit Care Med, 2015, 16(4): 428-39 [17] Low SY, Tan TT, Lee C, et al. Severe adenovirus pneumonia requiring extracorporeal membrane oxygenation support - Serotype 7 revisited[J]. Respir Med, 2013, 107(11): 1810-3 doi: 10.1016/j.rmed.2013.09.008 [18] de Blic J, Deschildre A, Chinet T. Post-infectious bronchiolitis obliterans[J]. Rev Mal Respir, 2013, 30(2): 152-60 doi: 10.1016/j.rmr.2012.10.600 [19] Castro-Rodriguez JA, Daszenies C, Garcia M, et al. Adenovirus pneumonia in infants and factors for developing bronchiolitis obliterans: a 5-year follow-up[J]. Pediatr Pulmonol, 2006, 41(10): 947-53 doi: 10.1002/(ISSN)1099-0496 [20] Colom AJ, Teper AM, Vollmer WM, et al. Risk factors for the development of bronchiolitis obliterans in children with bronchiolitis[J]. Thorax, 2006, 61(6): 503-6 doi: 10.1136/thx.2005.044909 [21] 颉雅苹. 儿童闭塞性细支气管炎18例临床特征分析[J]. 医学临床研究, 1994, 32(2): 51-2 [22] Rajkumar V, Chiang CS, Low JM, et al. Risk factors for severe adenovirus infection in children during an outbreak in Singapore[J]. Ann Acad Med Singapore, 2015, 44(2): 50-9 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 2476
- HTML全文浏览量: 810
- PDF下载量: 19
- 被引次数: 0